

Influence of age on seven putative prostate tumor markers: a cohort study in Chinese men
- PMID: 27048780
- PMCID: PMC5507094
- DOI: 10.4103/1008-682X.175787
Influence of age on seven putative prostate tumor markers: a cohort study in Chinese men
Abstract
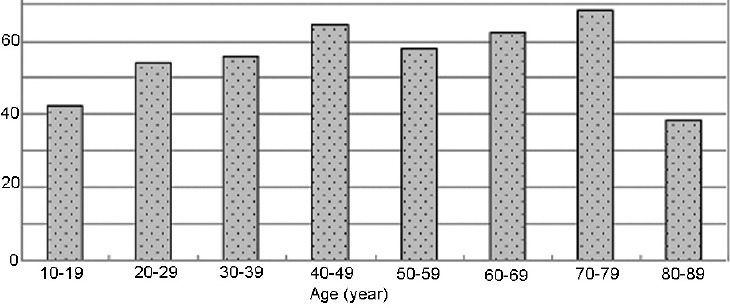
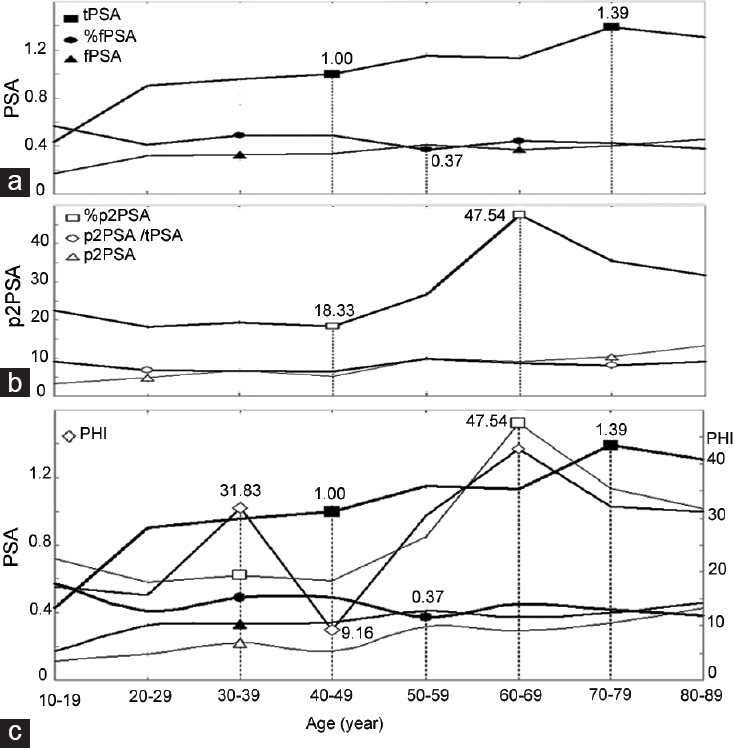
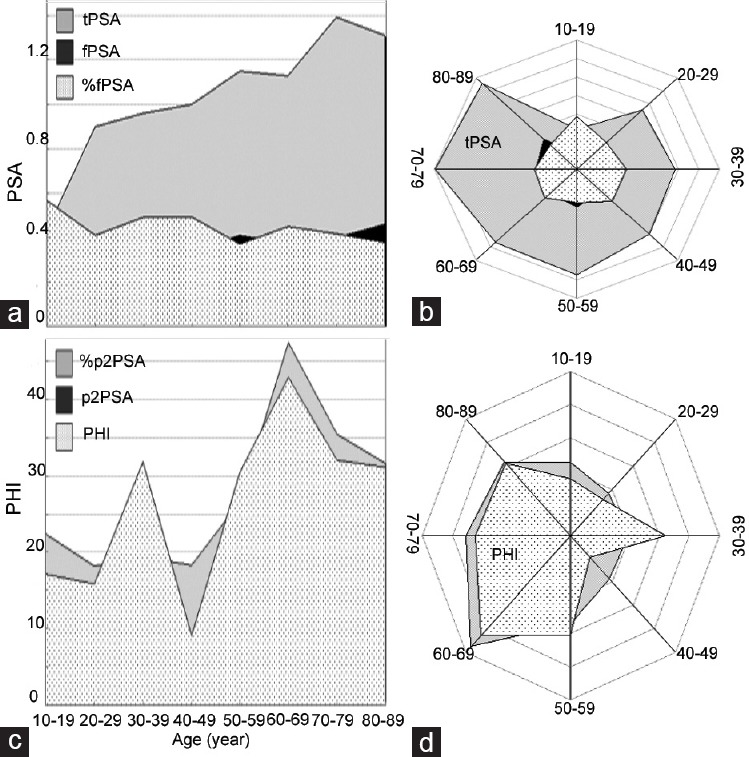
The accuracy and sensitivity of prostate-specific antigen (PSA) for prostate cancer diagnosis is often poor; however, the reasons for its inaccuracy have rarely been investigated, especially with respect to age. In this study, 476 healthy males, aged 10-89 years, were stratified into eight age groups, and levels of seven markers were determined: total PSA (tPSA), free PSA (fPSA), %fPSA, isoform [-2]proPSA (p2PSA), p2PSA/tPSA, %p2PSA, and the prostate health index (PHI). Both tPSA and fPSA levels increased with age. The tPSA level was highest (1.39 ng ml-1) at 70-79 years; %fPSA was highest (0.57 ng ml-1) at 10-19 years; and %p2PSA was lowest (18.33 ng ml-1) at 40-49 years. Both p2PSA and p2PSA/tPSA had relatively flat curves and showed no correlation with age (P = 0.222). PHI was a sensitive age-associated marker (P < 0.05), with two peaks and one trough. The coverage rates and radiance graphs of PHI and %p2PSA were more distinctive than those of tPSA and the other markers. In subjects older than 69 years, PHI and %p2PSA both began to decrease, approximately 10 years earlier than the decrease in tPSA. Our results suggest that the clinical diagnosis of prostate cancer using PSA should be investigated more comprehensively based on patient age. Moreover, %p2PSA and PHI could be considered as earlier markers that may be more suitable than PSA alone.
Figures
Similar articles
-
Serum isoform [-2]proPSA derivatives significantly improve prediction of prostate cancer at initial biopsy in a total PSA range of 2-10 ng/ml: a multicentric European study.Eur Urol. 2013 Jun;63(6):986-94. doi: 10.1016/j.eururo.2013.01.011. Epub 2013 Jan 24. Eur Urol. 2013. PMID: 23375961
-
Prostate-specific antigen (PSA) isoform p2PSA significantly improves the prediction of prostate cancer at initial extended prostate biopsies in patients with total PSA between 2.0 and 10 ng/ml: results of a prospective study in a clinical setting.Eur Urol. 2011 Aug;60(2):214-22. doi: 10.1016/j.eururo.2011.03.052. Epub 2011 Apr 5. Eur Urol. 2011. PMID: 21482022
-
Usefulness of the prostate health index in predicting the presence and aggressiveness of prostate cancer among Korean men: a prospective observational study.BMC Urol. 2021 Sep 16;21(1):131. doi: 10.1186/s12894-021-00897-2. BMC Urol. 2021. PMID: 34530786 Free PMC article.
-
Clinical performance of serum [-2]proPSA derivatives, %p2PSA and PHI, in the detection and management of prostate cancer.Am J Clin Exp Urol. 2014 Dec 25;2(4):343-50. eCollection 2014. Am J Clin Exp Urol. 2014. PMID: 25606581 Free PMC article. Review.
-
From prostate-specific antigen (PSA) to precursor PSA (proPSA) isoforms: a review of the emerging role of proPSAs in the detection and management of early prostate cancer.BJU Int. 2013 Oct;112(6):717-28. doi: 10.1111/j.1464-410X.2012.11329.x. Epub 2012 Jul 3. BJU Int. 2013. PMID: 22759214 Review.
Cited by
-
Establishment of reference intervals for serum [-2]proPSA (p2PSA), %p2PSA and prostate health index in healthy men.Onco Targets Ther. 2019 Aug 13;12:6453-6460. doi: 10.2147/OTT.S212340. eCollection 2019. Onco Targets Ther. 2019. PMID: 31616156 Free PMC article.
References
-
- Tosoian JJ, Ross AE, Sokoll LJ, Partin AW, Pavlovich CP. Urinary biomarkers for prostate cancer. Urol Clin North Am. 2016;43:17–38. - PubMed
-
- Loeb S. Time to replace prostate-specific antigen (PSA) with the prostate health index (PHI)? Yet more evidence that the PHI consistently outperforms PSA across diverse populations. BJU Int. 2015;115:500. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
