

CHAGASIC MENINGOENCEPHALITIS IN AN HIV INFECTED PATIENT WITH MODERATE IMMUNOSUPPRESSION: PROLONGED SURVIVAL AND CHALLENGES IN THE HAART ERA
- PMID: 27049711
- PMCID: PMC4727143
- DOI: 10.1590/S0036-46652015000600014
CHAGASIC MENINGOENCEPHALITIS IN AN HIV INFECTED PATIENT WITH MODERATE IMMUNOSUPPRESSION: PROLONGED SURVIVAL AND CHALLENGES IN THE HAART ERA
Abstract
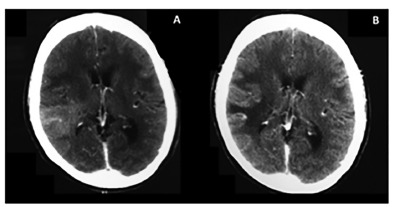
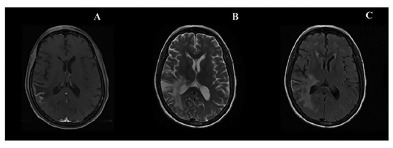
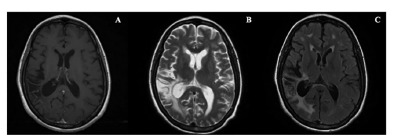
The reactivation of Chagas disease in HIV infected patients presents high mortality and morbidity. We present the case of a female patient with confirmed Chagasic meningoencephalitis as AIDS-defining illness. Interestingly, her TCD4+ lymphocyte cell count was 318 cells/mm3. After two months of induction therapy, one year of maintenance with benznidazol, and early introduction of highly active antiretroviral therapy (HAART), the patient had good clinical, parasitological and radiological evolution. We used a qualitative polymerase chain reaction for the monitoring of T. cruzi parasitemia during and after the treatment. We emphasize the potential value of molecular techniques along with clinical and radiological parameters in the follow-up of patients with Chagas disease and HIV infection. Early introduction of HAART, prolonged induction and maintenance of antiparasitic therapy, and its discontinuation are feasible, in the current management of reactivation of Chagas disease.
A reativação da doença de Chagas em pacientes com a infecção pelo HIV apresenta uma alta morbidade e mortalidade. Neste relato, apresentamos caso confirmado de meningoencefalite chagásica, como doença definidora de aids, em paciente com 318 linfócitos T-CD4+/mm3. Após 2 meses de tratamento seguido de um ano de profilaxia secundária com benzonidazol e início precoce de terapia antirretroviral (HAART), a paciente apresentou boa evolução clínica, parasitológica e radiológica. Utilizamos a reação em cadeia da polimerase qualitativa do T. cruzi, para monitorização da parasitemia por T. cruzi durante e após o tratamento. Ressaltamos o valor potencial das técnicas moleculares associadas aos parâmetros clínicos e radiológicos nos pacientes com doença de Chagas e infecção pelo HIV. A introdução precoce da terapia antirretroviral, a terapia antiparasitária prolongada, manutenção e descontinuação da mesma, são desafios atuais, embora possíveis, no manejo da reativação da doença de Chagas na era das terapias antirretrovirais de alta eficácia.
Conflict of interest statement
Figures
Similar articles
-
Prolonged survival and immune reconstitution after chagasic meningoencephalitis in a patient with acquired immunodeficiency syndrome.Rev Soc Bras Med Trop. 2006 Jan-Feb;39(1):85-8. doi: 10.1590/s0037-86822006000100018. Epub 2006 Feb 23. Rev Soc Bras Med Trop. 2006. PMID: 16501775
-
Chagasic meningoencephalitis: case report of a recently included AIDS-defining illness in Brazil.Rev Inst Med Trop Sao Paulo. 2004 Jul-Aug;46(4):199-202. doi: 10.1590/s0036-46652004000400005. Epub 2004 Sep 3. Rev Inst Med Trop Sao Paulo. 2004. PMID: 15361971
-
Trypanosoma cruzi meningoencephalitis in a patient with acquired immunodeficiency syndrome.Am J Trop Med Hyg. 2014 Jul;91(1):84-5. doi: 10.4269/ajtmh.14-0058. Epub 2014 Jun 2. Am J Trop Med Hyg. 2014. PMID: 24891470 Free PMC article.
-
Chagasic encephalitis in HIV patients: common presentation of an evolving epidemiological and clinical association.Lancet Infect Dis. 2009 May;9(5):324-30. doi: 10.1016/S1473-3099(09)70088-X. Lancet Infect Dis. 2009. PMID: 19393962 Review.
-
Reactivation of Chagas' disease in patients with AIDS: report of three new cases and review of the literature.Clin Infect Dis. 1997 Dec;25(6):1397-400. doi: 10.1086/516130. Clin Infect Dis. 1997. PMID: 9431385 Review.
Cited by
-
In vitro susceptibility to benznidazole, nifurtimox and posaconazole of Trypanosoma cruzi isolates from Paraguay.Biomedica. 2020 Dec 2;40(4):749-763. doi: 10.7705/biomedica.5187. Biomedica. 2020. PMID: 33275352 Free PMC article. English, Spanish.
References
-
- Almeida EA, Ramos AN, Júnior, Correia D, Shikanai-Yasuda MA. Rede Brasileira de Atenção e Estudos na co-infecção Trypanosoma cruzi/HIV e em outras condições de imunossupressão. Rev Soc Bras Med Trop. 2009;42:605–608. - PubMed
-
- Almeida EA, Lima JN, Lages-Silva E, Guariento ME, Aoki FH, Torres-Morales AE. Chagas' disease and HIV co-infection in patients without effective antiretroviral therapy: prevalence, clinical presentation and natural history. Trans R Soc Trop Med Hyg. 2010;104:447–452. - PubMed
-
- Almeida EA, Ramos AN, Júnior, Correia D, Shikanai-Yasuda MA. Co-infection Trypanosoma cruzi/HIV: systematic review (1980-2010) Rev Soc Bras Med Trop. 2011;44:762–770. - PubMed
-
- Amato V, Neto, Lopes MH, De Marchi CR, Silva MF. Tentativa de evidenciar o Trypanosoma cruzi no sangue periférico de pacientes com doença de Chagas, em fase crônica por meio do quantitative buffy coat (QBC) Rev Soc Bras Med Trop. 1998;31:231–233. - PubMed
-
- Brasil. Ministério da Saúde Recomendações para diagnóstico, tratamento e acompanhamento da co-infecção Trypanosoma cruzi: vírus da imunodeficiência humana. Rev Soc Bras Med Trop. 2006;39:392–341. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
