

Clostridium Perfringens Infection in a Febrile Patient with Severe Hemolytic Anemia
- PMID: 27049736
- PMCID: PMC4824343
- DOI: 10.12659/ajcr.895721
Clostridium Perfringens Infection in a Febrile Patient with Severe Hemolytic Anemia
Abstract
Background: Clostridium perfringens (C. perfringens) can cause various infections, including gas gangrene, crepitant cellulitis, and fasciitis. While C. perfringens sepsis is uncommon, it is often rapidly fatal because the alpha toxin of this bacterium induces massive intravascular hemolysis by disrupting red blood cell membranes.
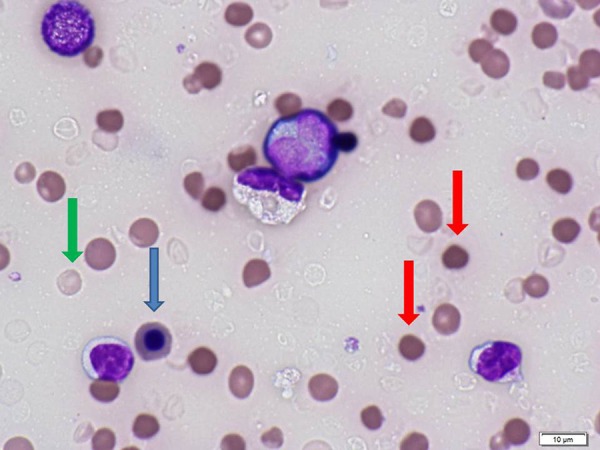
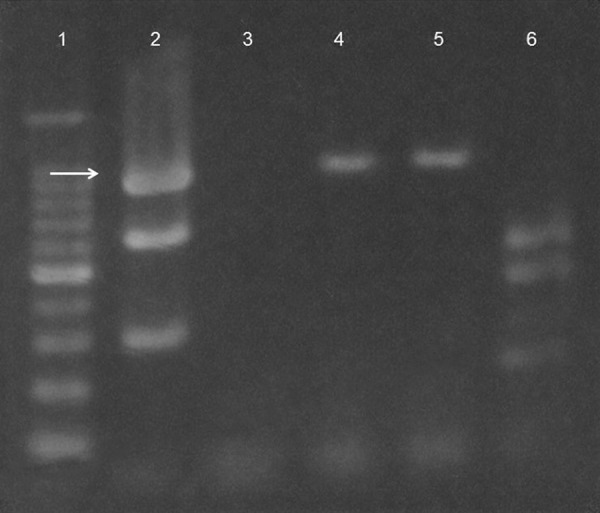
Case report: We present the case of a male patient with diabetes who developed a fatal liver abscess with massive intravascular hemolysis and septic shock caused by toxigenic C. perfringens. The peripheral blood smear showed loss of central pallor, with numerous spherocytes. Multiplex PCR only detected expression of the cpa gene, indicating that the pathogen was C. perfringens type A.
Conclusions: C. perfringens infection should be considered in a febrile patient who has severe hemolytic anemia with a very low MCV, hemolyzed blood sample, and negative Coombs test. The characteristic peripheral blood smear findings may facilitate rapid diagnosis.
Figures

References
-
- van Bunderen CC, Bomers MK, Wesdorp E, et al. Clostridium perfringens septicaemia with massive intravascular haemolysis: A case report and review of the literature. Neth J Med. 2010;68:343–46. - PubMed
-
- Simon TG, Bradley J, Jones A, et al. Massive intravascular hemolysis from Clostridium perfringens septicemia: A review. J Intensive Care Med. 2014;29:327–33. - PubMed
-
- Craven CM. Fatal Clostridium perfringens septicemia associated with gastrointestinal arteriovenous malformation. Arch Pathol Lab Med. 1989;113:534–35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
