

Preoperative Cholangitis and Future Liver Remnant Volume Determine the Risk of Liver Failure in Patients Undergoing Resection for Hilar Cholangiocarcinoma
- PMID: 27049784
- PMCID: PMC4925184
- DOI: 10.1016/j.jamcollsurg.2016.01.060
Preoperative Cholangitis and Future Liver Remnant Volume Determine the Risk of Liver Failure in Patients Undergoing Resection for Hilar Cholangiocarcinoma
Abstract
Background: The highest mortality rates after liver surgery are reported in patients who undergo resection for hilar cholangiocarcinoma (HCCA). In these patients, postoperative death usually follows the development of hepatic insufficiency. We sought to determine the factors associated with postoperative hepatic insufficiency and death due to liver failure in patients undergoing hepatectomy for HCCA.
Study design: This study included all consecutive patients who underwent hepatectomy with curative intent for HCCA at 2 centers, from 1996 through 2013. Preoperative clinical and operative data were analyzed to identify independent determinants of hepatic insufficiency and liver failure-related death.
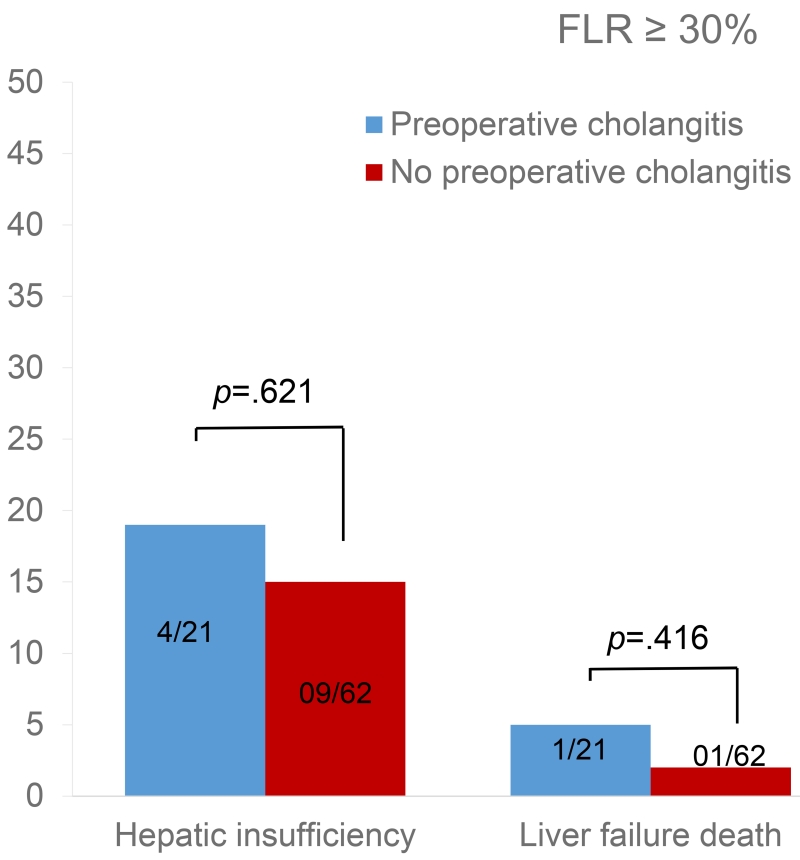
Results: The study included 133 patients with right or left major (n = 67) or extended (n = 66) hepatectomy. Preoperative biliary drainage was performed in 98 patients and was complicated by cholangitis in 40 cases. In all these patients, cholangitis was controlled before surgery. Major (Dindo III to IV) postoperative complications occurred in 73 patients (55%), with 29 suffering from hepatic insufficiency. Fifteen patients (11%) died within 90 days after surgery, 10 of them from liver failure. On multivariate analysis, predictors of postoperative hepatic insufficiency (all p < 0.05) were preoperative cholangitis (odds ratio [OR] 3.2), future liver remnant (FLR) volume < 30% (OR 3.5), preoperative total bilirubin level >3 mg/dL (OR 4), and albumin level < 3.5 mg/dL (OR 3.3). Only preoperative cholangitis (OR 7.5, p = 0.016) and FLR volume < 30% (OR 7.2, p = 0.019) predicted postoperative liver failure-related death.
Conclusions: Preoperative cholangitis and insufficient FLR volume are major determinants of hepatic insufficiency and postoperative liver failure-related death. Given the association between biliary drainage and cholangitis, the preoperative approach to patients with HCCA should be optimized to minimize the risk of cholangitis.
Copyright © 2016 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Discussion.J Am Coll Surg. 2016 Jul;223(1):97-8. doi: 10.1016/j.jamcollsurg.2016.04.033. J Am Coll Surg. 2016. PMID: 27345905 No abstract available.
-
Importance of Preoperative Optimization in Resection of Perihilar Cholangiocarcinoma.J Am Coll Surg. 2016 Jul;223(1):208-9. doi: 10.1016/j.jamcollsurg.2016.04.007. J Am Coll Surg. 2016. PMID: 27345924 No abstract available.
References
-
- Vauthey JN, Blumgart LH. Recent advances in the management of cholangiocarcinomas. Semin Liver Dis. 1994;14:109–114. - PubMed
-
- Nagino M, Kamiya J, Uesaka K, et al. Complications of hepatectomy for hilar cholangiocarcinoma. World J Surg. 2001;25:1277–1283. - PubMed
-
- Smith RC, Pooley M, George CR, Faithful GR. Preoperative percutaneous transhepatic internal drainage in obstructive jaundice: a randomized, controlled trial examining renal function. Surgery. 1985;97:641–648. - PubMed
-
- Imamura H, Shimada R, Kubota M, et al. Preoperative portal vein embolization: an audit of 84 patients. Hepatology. 1999;29:1099–1105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
