

Dynamic Risk Stratification of Patient Long-Term Outcome After Pulmonary Endarterectomy: Results From the United Kingdom National Cohort
- PMID: 27052413
- PMCID: PMC5860739
- DOI: 10.1161/CIRCULATIONAHA.115.019470
Dynamic Risk Stratification of Patient Long-Term Outcome After Pulmonary Endarterectomy: Results From the United Kingdom National Cohort
Abstract
Background: Chronic thromboembolic pulmonary hypertension results from incomplete resolution of pulmonary emboli. Pulmonary endarterectomy (PEA) is potentially curative, but residual pulmonary hypertension following surgery is common and its impact on long-term outcome is poorly understood. We wanted to identify factors correlated with poor long-term outcome after surgery and specifically define clinically relevant residual pulmonary hypertension post-PEA.
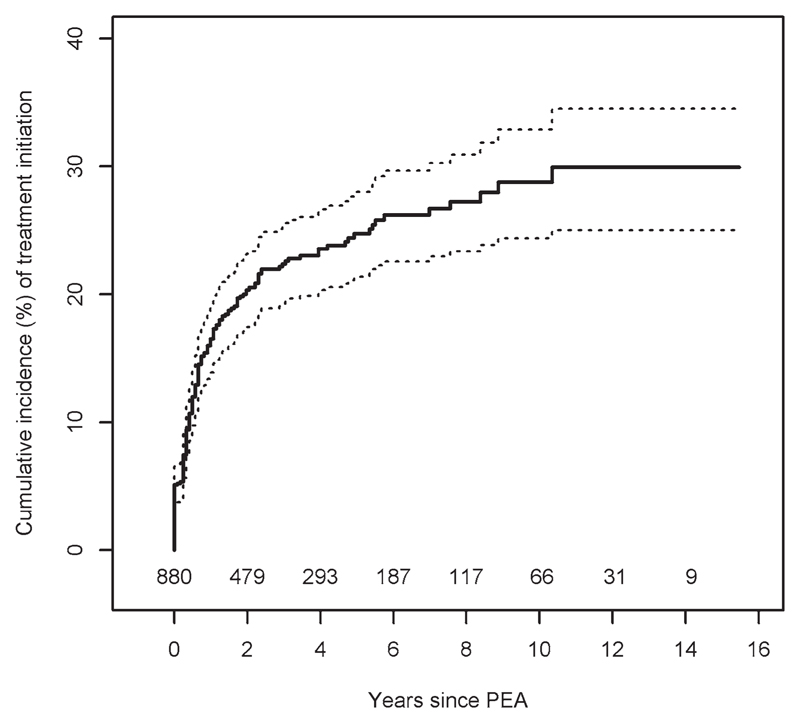
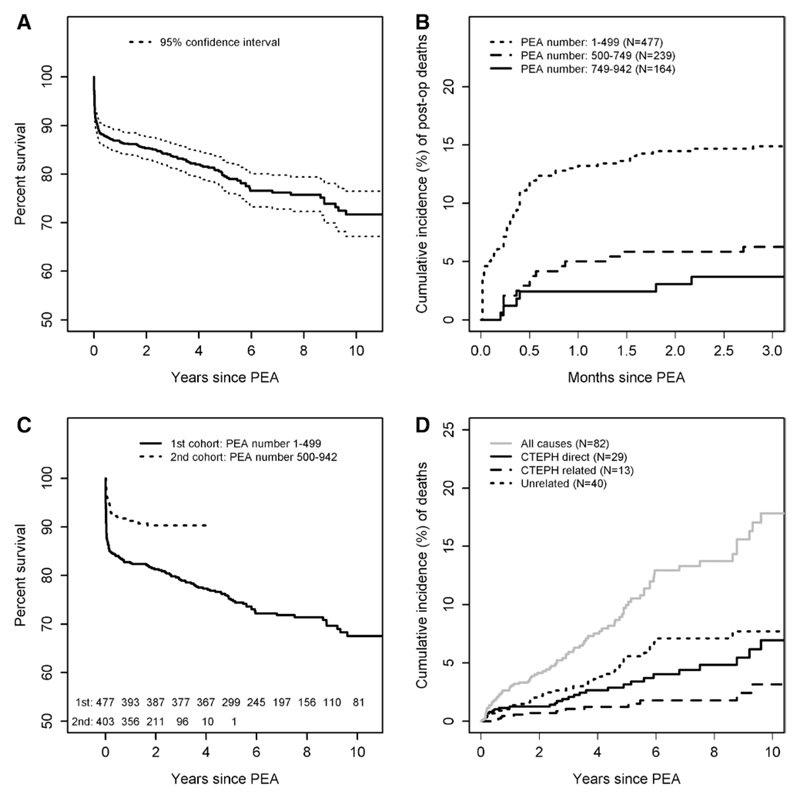
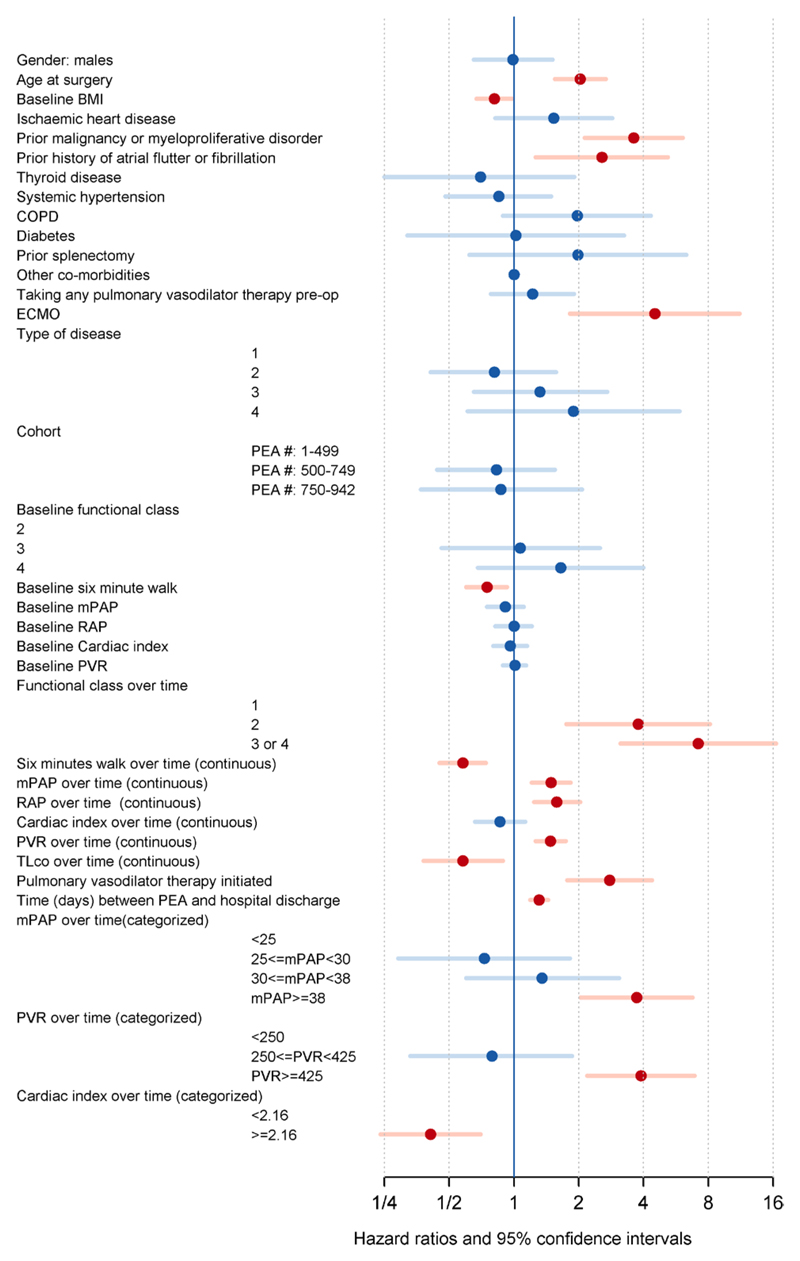
Methods and results: Eight hundred eighty consecutive patients (mean age, 57 years) underwent PEA for chronic thromboembolic pulmonary hypertension. Patients routinely underwent detailed reassessment with right heart catheterization and noninvasive testing at 3 to 6 months and annually thereafter with discharge if they were clinically stable at 3 to 5 years and did not require pulmonary vasodilator therapy. Cox regressions were used for survival (time-to-event) analyses. Overall survival was 86%, 84%, 79%, and 72% at 1, 3, 5, and 10 years for the whole cohort and 91% and 90% at 1 and 3 years for the recent half of the cohort. The majority of patient deaths after the perioperative period were not attributable to right ventricular failure (chronic thromboembolic pulmonary hypertension). At reassessment, a mean pulmonary artery pressure of ≥30 mm Hg correlated with the initiation of pulmonary vasodilator therapy post-PEA. A mean pulmonary artery pressure of ≥38 mm Hg and pulmonary vascular resistance ≥425 dynes·s(-1)·cm(-5) at reassessment correlated with worse long-term survival.
Conclusions: Our data confirm excellent long-term survival and maintenance of good functional status post-PEA. Hemodynamic assessment 3 to 6 months and 12 months post-PEA allows stratification of patients at higher risk of dying of chronic thromboembolic pulmonary hypertension and identifies a level of residual pulmonary hypertension that may guide the long-term management of patients postsurgery.
Keywords: endarterectomy; hypertension, pulmonary; pulmonary embolism; survival.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Dr Cannon has received speaker fees and honoraria from Actelion and GSK. Dr Kiely has received speaker fees, honoraria and has been on advisory boards for Actelion, Bayer, GSK, Pfizer and United Therapeutics and has received research grants from Actelion, Pfizer and Bayer. Dr Toshner has received speaker fees and honoraria from Actelion, GSK and Bayer and research grants from Bayer. Dr Condliffe has received speaker fees and honoraria from Actelion and GSK, research grants from Actelion, Pfizer and Bayer, and is on advisory boards for Actelion and Bayer. Dr Sheares has received honoraria from Actelion, GSK, Bayer and Pfizer. Dr Taboada has received honoraria from Actelion, Bayer, Pfizer, Lilly and GSK. Dr Elliot has received honoraria from Actelion and Bayer, has been on advisory boards for Actelion and GSK, and has received research grants from Actelion, Bayer and Pfizer. Dr Gibbs has received speaker fees and honoraria from Actelion, Bayer, GSK, Lilly, Pfizer and United Therapeutics, has received research grants from Actelion and United Therapeutics and is on advisory boards for Actelion, Gilead, Lilly and Novartis. Dr Howard has received speaker fees and honoraria from Actelion, GSK and Pfizer and is on advisory boards for Actelion, Bayer, GSK, Pfizer and Novartis. Dr Lordan has received speaker fees and honoraria from Bayer, Pfizer and Eli Lilly, and is on advisory boards for Bayer. Dr Corris has received research grants from Actelion, Pfizer, and GSK, and is on advisory boards for Actelion, Pfizer, Bayer, GSK, Novartis, and Lilly. Dr Johnson has received speaker fees from Actelion and GSK and honoraria from Actelion, Bayer, GSK, and Pfizer. Dr Peacock has received speaker fees, honoraria, and research grants from Actelion, Pfizer, and GSK, and is on advisory boards for Actelion, Bayer, GSK, Pfizer and Lilly. Dr Schreiber has received honoraria from Actelion, GSK, and Pfizer. Dr Coghlan has received honoraria for lecturing from Actelion, GSK, Pfizer, and Lilly, and is on advisory boards for Actelion, Bayer, and Pfizer. Dr Dimopoulos has received speaker fees from Actelion, honoraria from Actelion and GSK, and research grants from Actelion, GSK, and Pfizer. Dr Wort has received speaker fees and honoraria from Actelion and Pfizer, has received research grants from Actelion, Pfizer, and Bayer, and is on advisory boards for Pfizer, GSK, Novartis, and Bayer. Dr Gaine has received speaker fees and honoraria and is on advisory boards for Actelion, GSK, and Pfizer. Dr Moledina has received speaker fees and honoraria from Actelion. Dr Jenkins has received honoraria for lecturing and consultancy from Actelion, Bayer, and GSK. Dr Pepke-Zaba has received honoraria for lecturing and consulting from Bayer, Actelion, and GSK, is on advisory boards for Actelion, Pfizer, Bayer, GSK, and United Therapeutics, and her institution has received educational and research grants from Actelion, Bayer, and GSK. The other authors report no conflicts.
Figures
Comment in
-
Letter by Kataoka et al Regarding Article, "Dynamic Risk Stratification of Patient Long-Term Outcome After Pulmonary Endarterectomy: Results From the United Kingdom National Cohort".Circulation. 2016 Oct 4;134(14):e299-e300. doi: 10.1161/CIRCULATIONAHA.116.023550. Circulation. 2016. PMID: 27698052 No abstract available.
-
Response by Cannon and Pepke-Zaba to Letter Regarding Article, "Dynamic Risk Stratification of Patient Long-Term Outcome After Pulmonary Endarterectomy: Results From the United Kingdom National Cohort".Circulation. 2016 Oct 4;134(14):e301-e302. doi: 10.1161/CIRCULATIONAHA.116.024416. Circulation. 2016. PMID: 27698053 No abstract available.
References
-
- Pepke-Zaba J, Delcroix M, Lang I, Mayer E, Jansa P, Ambroz D, Treacy C, D’Armini AM, Morsolini M, Snijder R, Bresser P, et al. Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation. 2011;124:1973–1981. doi: 10.1161/CIRCULATIONAHA.110.015008. - DOI - PubMed
-
- Riedel M, Stanek V, Widimsky J, Prerovsky I. Longterm follow-up of patients with pulmonary thromboembolism. Late prognosis and evolution of hemodynamic and respiratory data. Chest. 1982;81:151–158. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
