

Establishing a National Maternal Morbidity Outcome Indicator in England: A Population-Based Study Using Routine Hospital Data
- PMID: 27054761
- PMCID: PMC4824476
- DOI: 10.1371/journal.pone.0153370
Establishing a National Maternal Morbidity Outcome Indicator in England: A Population-Based Study Using Routine Hospital Data
Abstract
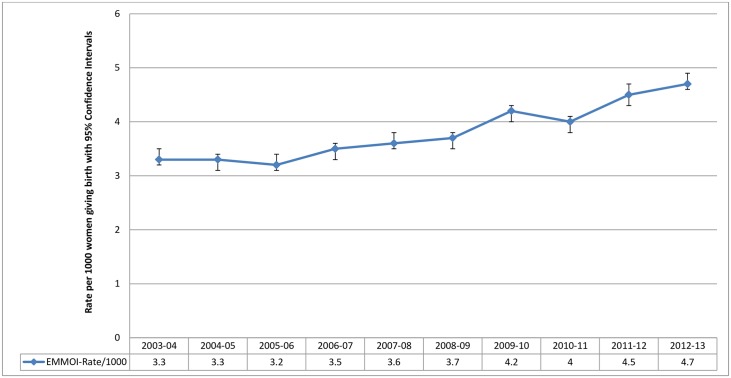
Introduction: As maternal deaths become rarer, monitoring near-miss or severe maternal morbidity becomes important as a tool to measure changes in care quality. Many calls have been made to use routinely available hospital administration data to monitor the quality of maternity care. We investigated 1) the feasibility of developing an English Maternal Morbidity Outcome Indicator (EMMOI) by reproducing an Australian indicator using routinely available hospital data, 2) the impact of modifications to the indicator to address potential data quality issues, 3) the reliability of the indicator.
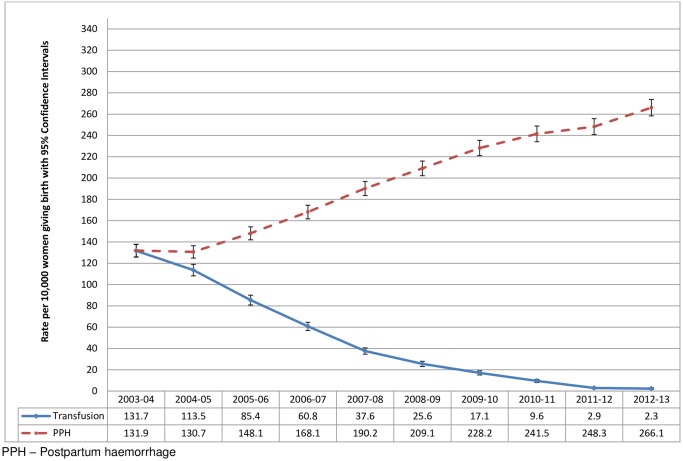
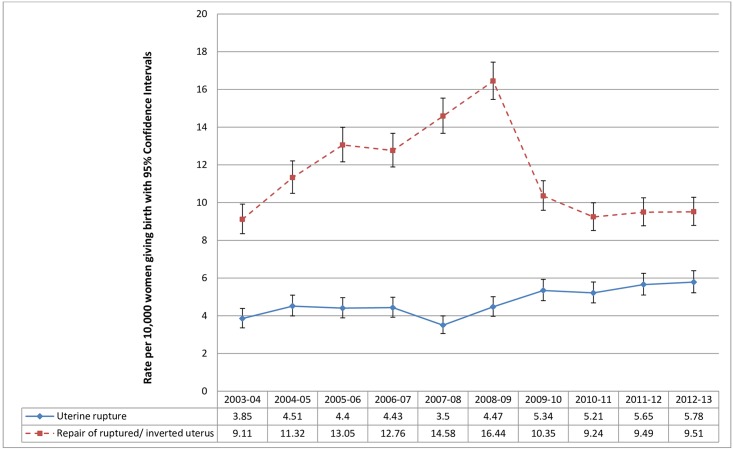
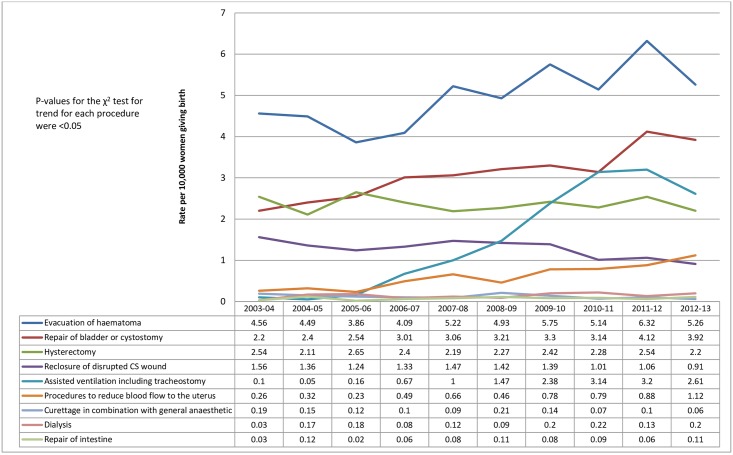
Methods: We used data from 6,389,066 women giving birth in England from April 2003 to March 2013 available in the Hospital Episode Statistics (HES) database of the Health and Social care Information centre (HSCIC). A composite indicator, EMMOI, was generated from the diagnoses and procedure codes. Rates of individual morbid events included in the EMMOI were compared with the rates in the UK reported by population-based studies.
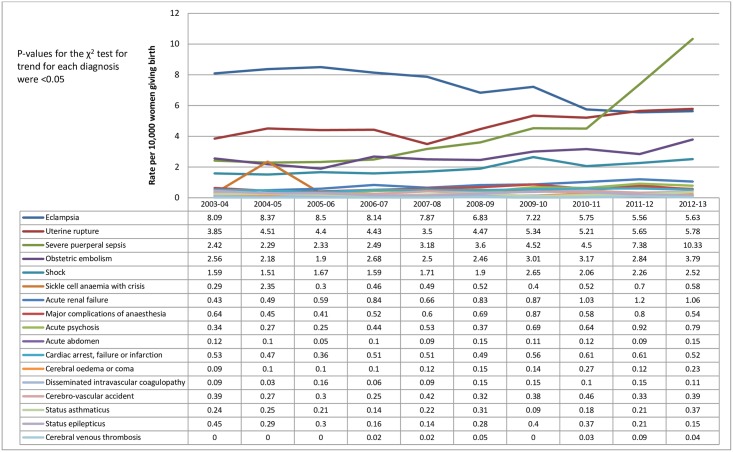
Results: EMMOI included 26 morbid events (17 diagnosis and 9 procedures). Selection of the individual morbid events was guided by the Australian indicator and published literature for conditions associated with maternal morbidity and mortality in the UK, but was mainly driven by the quality of the routine hospital data. Comparing the rates of individual morbid events of the indicator with figures from population-based studies showed that the possibility of false positive and false negative cases cannot be ruled out.
Conclusion: While routine English hospital data can be used to generate a composite indicator to monitor trends in maternal morbidity during childbirth, the quality and reliability of this monitoring indicator depends on the quality of the hospital data, which is currently inadequate.
Conflict of interest statement
Figures
References
-
- Hollowel J, Puddicombe D, Rowe R, Linsell L, Hardy P, Stewart M, et al. (2011) The Birthplace national prospective cohort study: perinatal and maternal outcomes by planned place of birth. Birthplace in England research programme. Final report part 4. NIHR Service Delivery and Organisation programme.
-
- Lim SS, Dandona L, Hoisington JA, James SL, Hogan MC, Gakidou E (2010) India's Janani Suraksha Yojana, a conditional cash transfer programme to increase births in health facilities: an impact evaluation. The Lancet 375: 2009–2023. - PubMed
-
- Paul BK, Rumsey DJ (2002) Utilization of health facilities and trained birth attendants for childbirth in rural Bangladesh: an empirical study. Social science & medicine 54: 1755–1765. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
