

Does delay in referral of proliferative diabetic retinopathy from the diabetic eye screening programme lead to visual loss?
- PMID: 27055673
- PMCID: PMC4906462
- DOI: 10.1038/eye.2016.56
Does delay in referral of proliferative diabetic retinopathy from the diabetic eye screening programme lead to visual loss?
Abstract
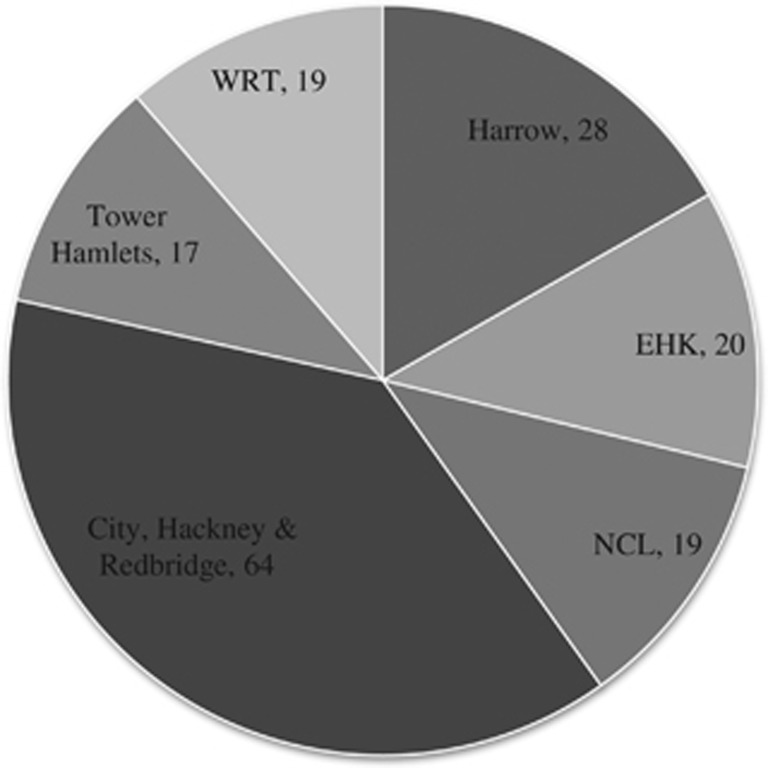
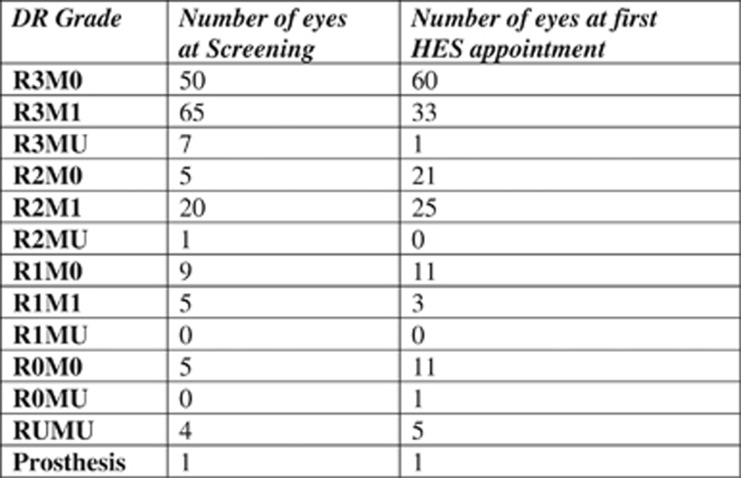
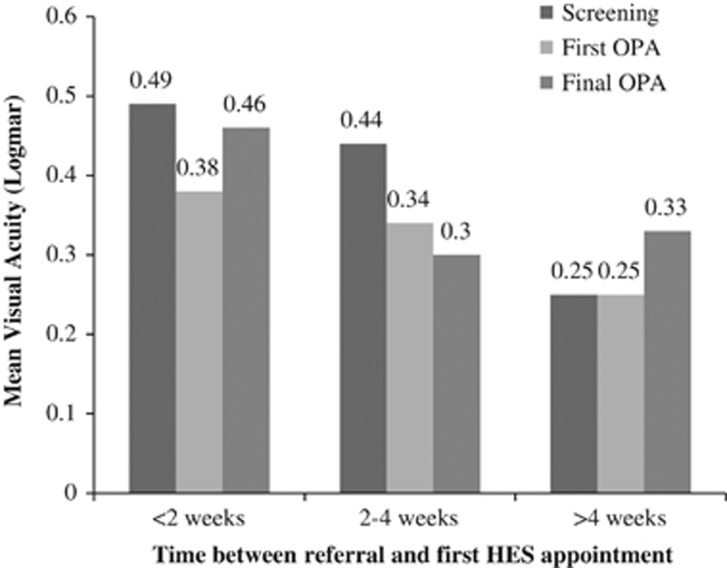
AimsTo ascertain the effect on visual acuity (VA) of a delay in Hospital Eye Service (HES) consultation for patients referred with proliferative diabetic retinopathy (PDR; R3) from the Diabetic Eye Screening Programme (DESP).MethodsAll patients referred to Moorfields Eye Hospital from DESP between April and December 2013 with a referral diagnosis of PDR in at least one eye were eligible. Screening programme VA was compared with VA at first HES appointment and final follow-up appointment. Reasons for any VA loss were noted.ResultsA total of 86 patients were included. Of these, 28 (33%) were seen in more than 4 weeks after their DESP referral. At first HES appointment, 39 (45%) patients were graded as having active PDR in at least one eye. Delay in referral did not significantly predict the likelihood of vision loss in all patients referred (χ(2), P=0.49) or in just those patients with a definitive HES diagnosis of active PDR (χ(2), P=1.00). In only 3 patients with active PDR was a delay in presentation thought to have led directly to VA loss.ConclusionsThere may be minimal short-term visual consequence in several weeks of delayed referral for many patients with a diagnosis of R3. However, the national guidance remains important. This is due to the occasional patient at very high risk of vision loss and the many gains for the patients in terms of time to properly assess medical and ocular conditions and counsel and consent them for treatment where necessary.
Figures
References
-
- NHS Diabetic Eye Screening Programme. Available at http://diabeticeye.screening.nhs.uk/. Accessed 2 January 2015.
-
- Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie House classification. ETDRS report number 10. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 1991; 98(5 Suppl): 786–806. - PubMed
-
- Early photocoagulation for diabetic retinopathy. ETDRS Report Number 9. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 1991; 98: 766–785. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
