

Fat-Soluble Vitamins: Clinical Indications and Current Challenges for Chromatographic Measurement
- PMID: 27057076
- PMCID: PMC4810759
Fat-Soluble Vitamins: Clinical Indications and Current Challenges for Chromatographic Measurement
Abstract
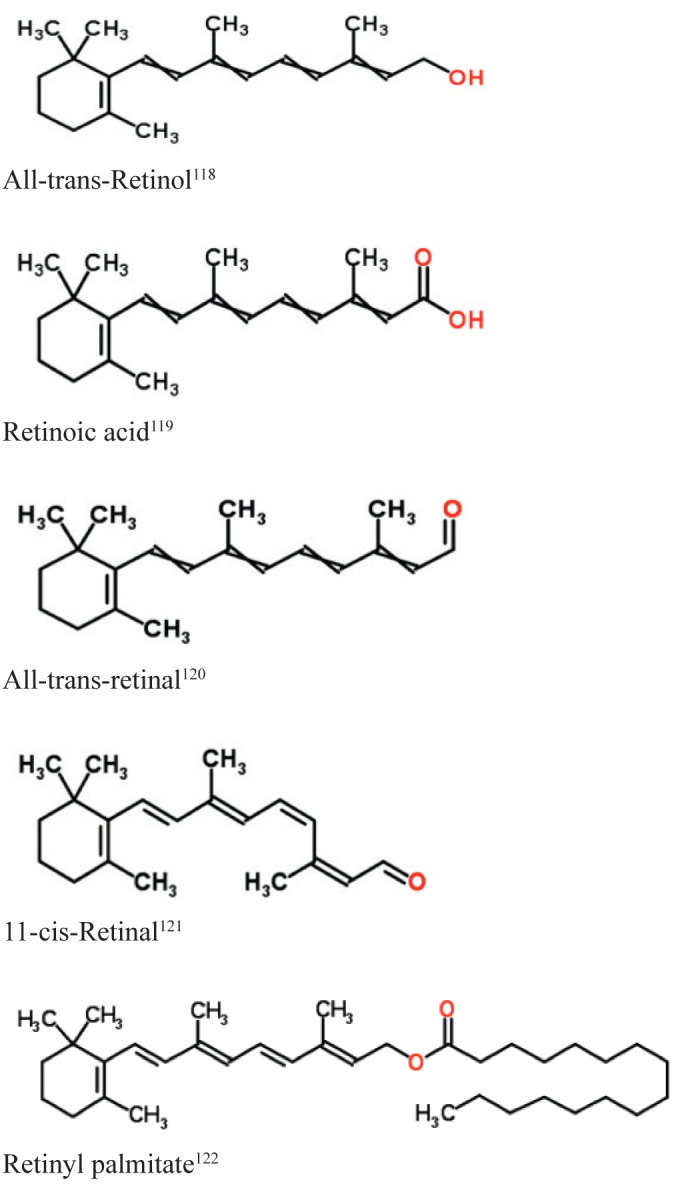
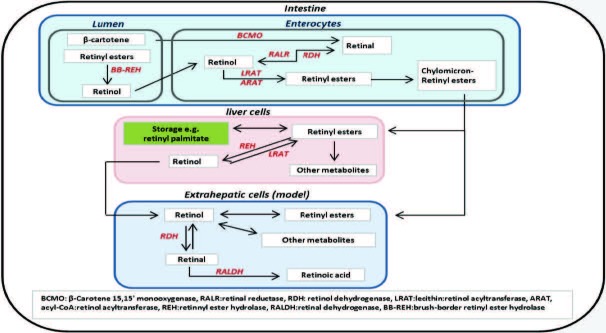
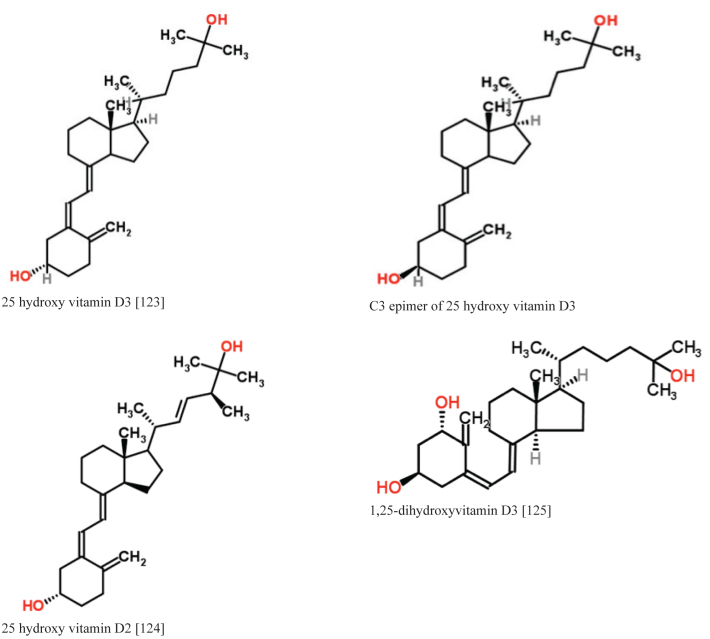
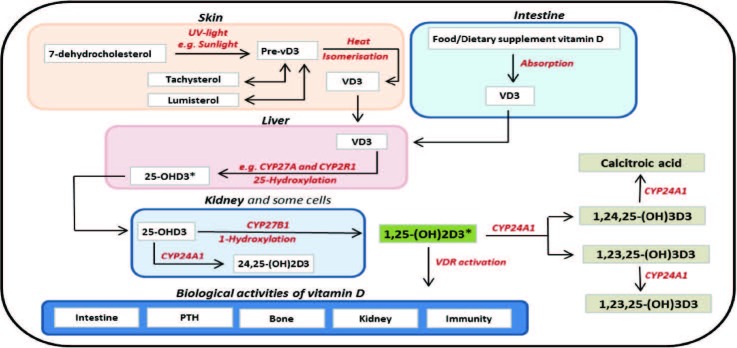
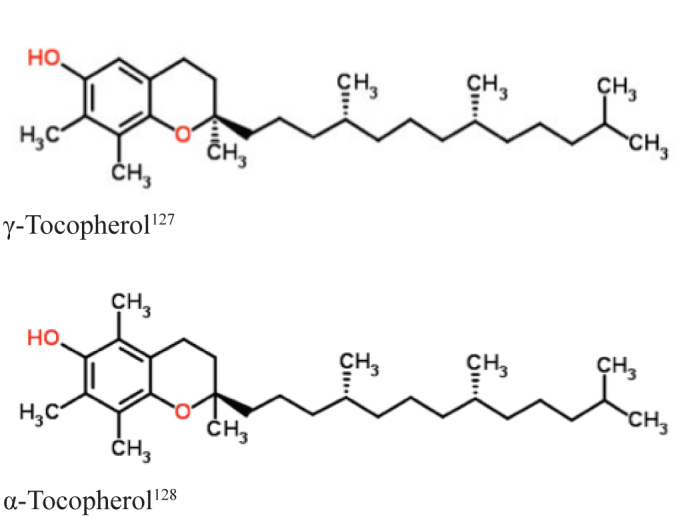
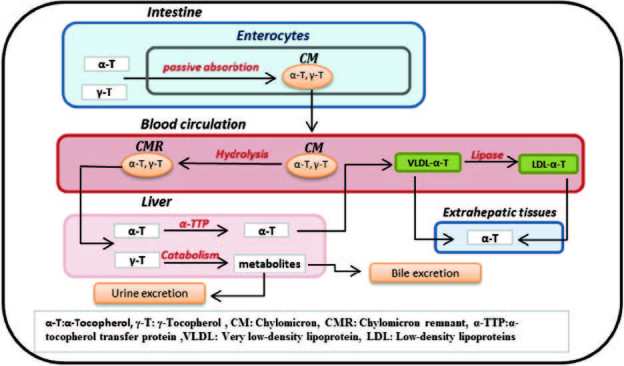
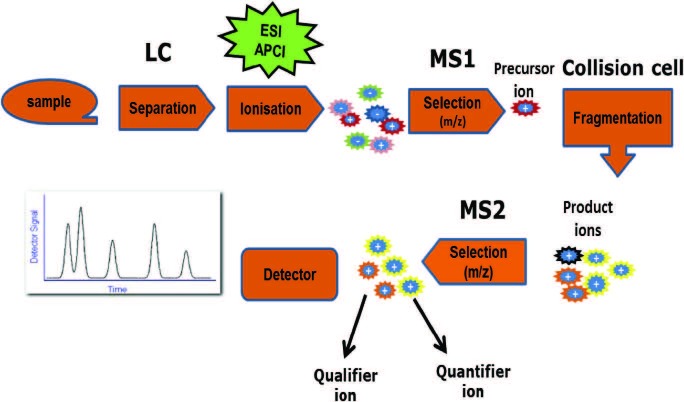
Fat-soluble vitamins, including vitamins A, D and E, are required for a wide variety of physiological functions. Over the past two decades, deficiencies of these vitamins have been associated with increased risk of cancer, type II diabetes mellitus and a number of immune system disorders. In addition, there is increasing evidence of interactions between these vitamins, especially between vitamins A and D. As a result of this enhanced clinical association with disease, translational clinical research and laboratory requests for vitamin measurements have significantly increased. These laboratory requests include measurement of 25-OHD (vitamin D), retinol (vitamin A) and α-tocopherol (vitamin E); the most accepted blood indicators for the assessment of body fat-soluble vitamin (FSV) status. There are significant obstacles to precise FSV measurement in blood. These obstacles include their physical and chemical properties, incomplete standardisation of measurement and limitations in the techniques that are currently used for quantification. The aim of this review is to briefly outline the metabolism and interactions of FSV as a prelude to identifying the current challenges for the quantification of blood vitamins A, D and E.
Figures
References
-
- Plum LA, DeLuca HF. Vitamin D, disease and therapeutic opportunities. Nat Rev Drug Discov. 2010;9:941–55. - PubMed
-
- Stephensen CB. Vitamin A, infection, and immune function. Annu Rev Nutr. 2001;21:167–92. - PubMed
-
- Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80(Suppl):1678S–88S. - PubMed
-
- Herrmann M. The measurement of 25-hydroxy vitamin D - an analytical challenge. Clin Chem Lab Med. 2012;50:1873–5. - PubMed
-
- Ross C. Vitamin A and carotenoids. In: Shils ME, Shike M, editors. Modern Nutrition in Health and Disease. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2006. pp. 305–27.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous