

Case Report: Acute Cerebellar Thrombosis in an Adult Patient with IgM Nephropathy
- PMID: 27057296
- PMCID: PMC4814013
- DOI: 10.14797/mdcj-11-4-247
Case Report: Acute Cerebellar Thrombosis in an Adult Patient with IgM Nephropathy
Abstract
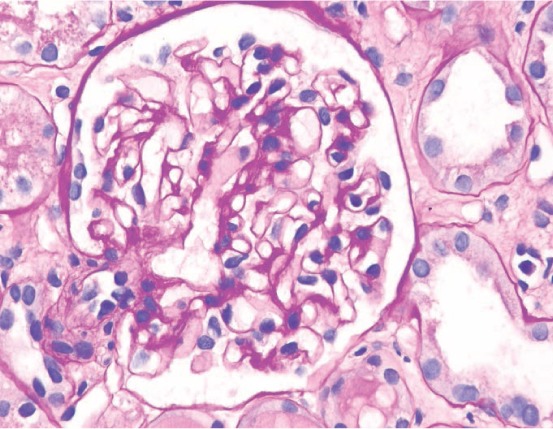
IgM nephropathy is a relatively rare cause of idiopathic nephrotic syndrome.1 It was initially described by van de Putte,2 then by Cohen and Bhasin in 1978, as a distinctive feature of mesangial proliferative glomerulonephritis.2 It is typically characterized by diffuse IgM deposits on the glomeruli and diffuse mesangial hypercellularity. Little is known about the pathogenesis and treatment of this disease.1,3 We describe a patient who presented with nonspecific symptoms of epigastric pain, nausea, and early satiety. Abdominal imaging and endoscopies were unremarkable. She was found to have significant proteinuria (6.4 g/24 hours), hyperlipidemia, and edema consistent with a diagnosis of nephrotic syndrome. Kidney biopsy was performed and confirmed an IgM nephropathy. Less than 2 weeks after her diagnosis of IgM nephropathy, she presented with an acute cerebellar stroke. Thrombophilia is a well-known complication of nephrotic syndrome, but a review of the literature failed to show an association between IgM nephropathy and acute central nervous system thrombosis.
Keywords: IgM nephropathy; cerebellar thrombosis; thromboembolic events.
Figures



Similar articles
-
IgM nephropathy complicated by cerebral venous sinus thrombosis: a case study.BMC Nephrol. 2020 Sep 7;21(1):390. doi: 10.1186/s12882-020-02048-5. BMC Nephrol. 2020. PMID: 32894094 Free PMC article.
-
A case report of immunoglobulin M nephropathy manifesting as crescentic glomerulonephritis and nephrotic syndrome in an adult.BMC Nephrol. 2019 Aug 27;20(1):335. doi: 10.1186/s12882-019-1528-2. BMC Nephrol. 2019. PMID: 31455257 Free PMC article.
-
Case of immunoglobulin M nephropathy in a patient with neurofibromatosis type 1.Nephrology (Carlton). 2015 Sep;20(9):666-7. doi: 10.1111/nep.12487. Nephrology (Carlton). 2015. PMID: 26278121 No abstract available.
-
Attending rounds: an older patient with nephrotic syndrome.Clin J Am Soc Nephrol. 2012 Apr;7(4):665-70. doi: 10.2215/CJN.12771211. Epub 2012 Mar 8. Clin J Am Soc Nephrol. 2012. PMID: 22403277 Review.
-
A male with angioimmunoblastic T-cell lymphoma and proliferative glomerulonephritis.Ann Hematol. 2004 Jul;83(7):455-9. doi: 10.1007/s00277-003-0828-5. Epub 2004 Mar 18. Ann Hematol. 2004. PMID: 15034757 Review.
References
-
- van de Putte LB, de la Riviere GB, van Breda Vriesman PJ. Recurrent or persistent hematuria. Sign of mesangial immune-complex deposition. N Engl J Med. 1974 May 23;290(21):1165–70. - PubMed
-
- de Seigneux S, Martin PY. Management of patients with nephrotic syndrome. Swiss Med Wkly. 2009 Jul 25;139(29–30):416–22. - PubMed
-
- Mokhtar GA. IgM nephropathy: clinical picture and pathological findings in 36 patients. Saudi J Kidney Dis Transpl. 2011 Sep;22(5):969–75. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
