

A Current Review of the Meniscus Imaging: Proposition of a Useful Tool for Its Radiologic Analysis
- PMID: 27057352
- PMCID: PMC4766355
- DOI: 10.1155/2016/8329296
A Current Review of the Meniscus Imaging: Proposition of a Useful Tool for Its Radiologic Analysis
Abstract
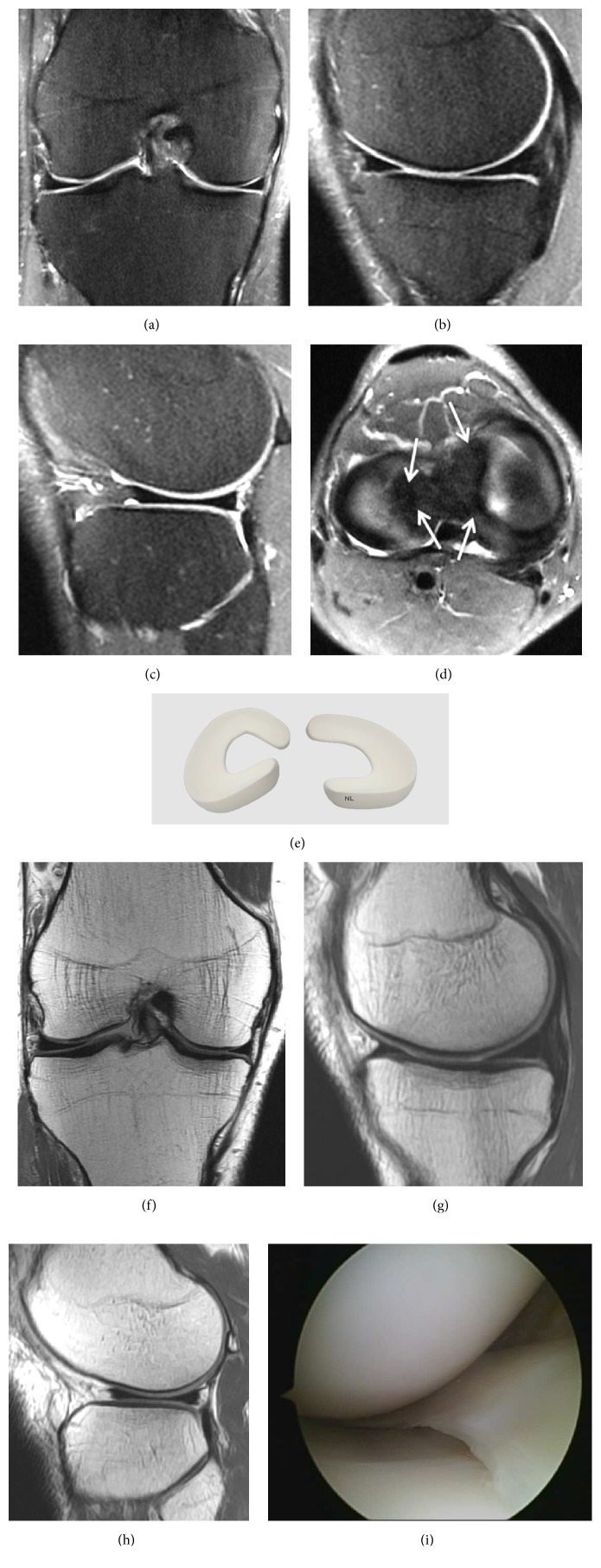
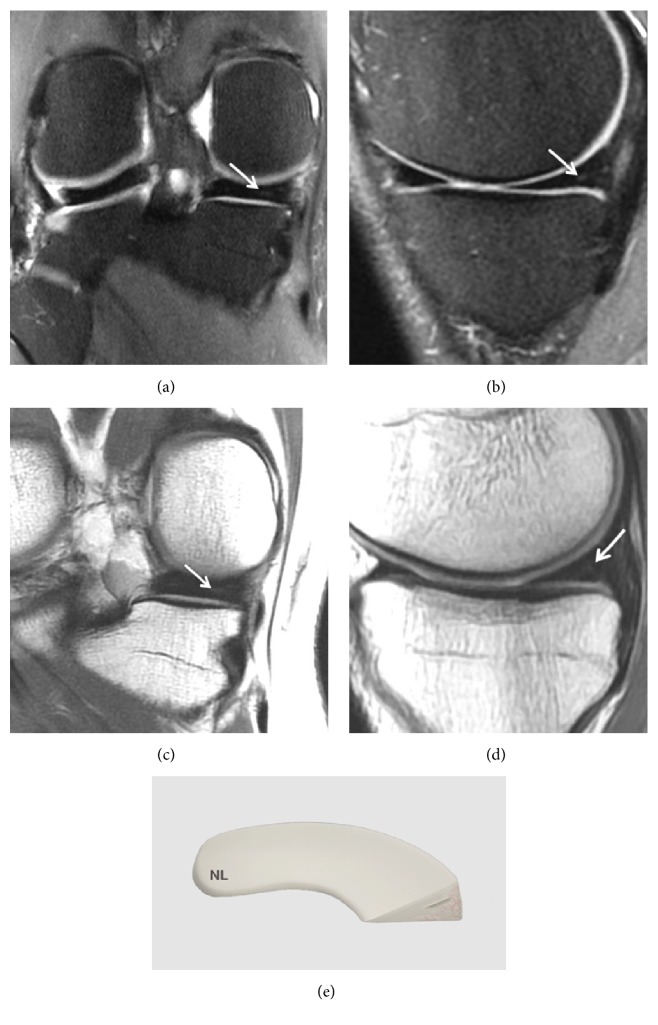
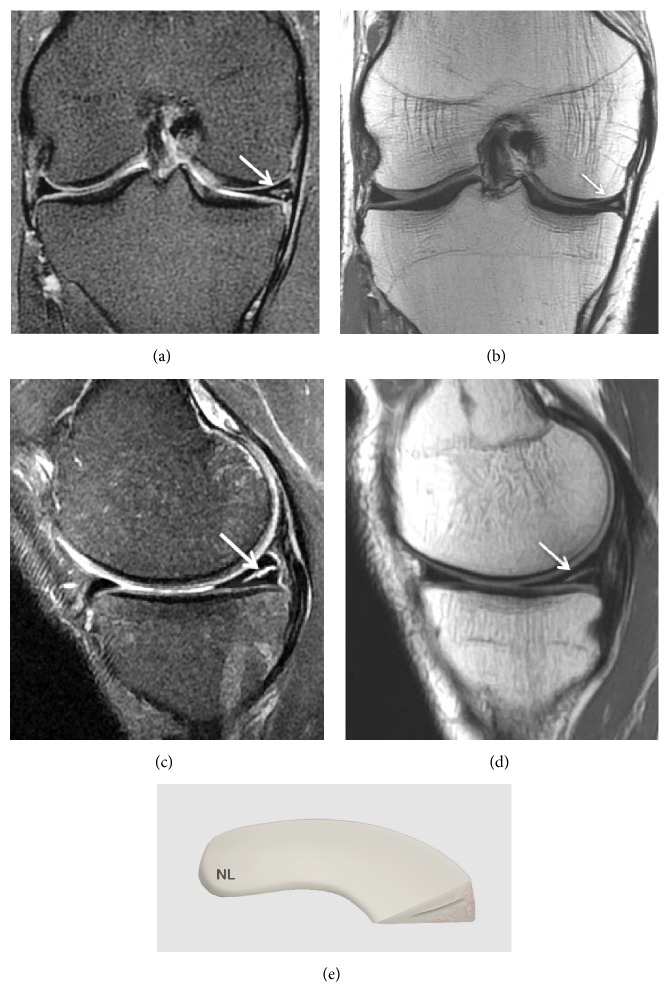
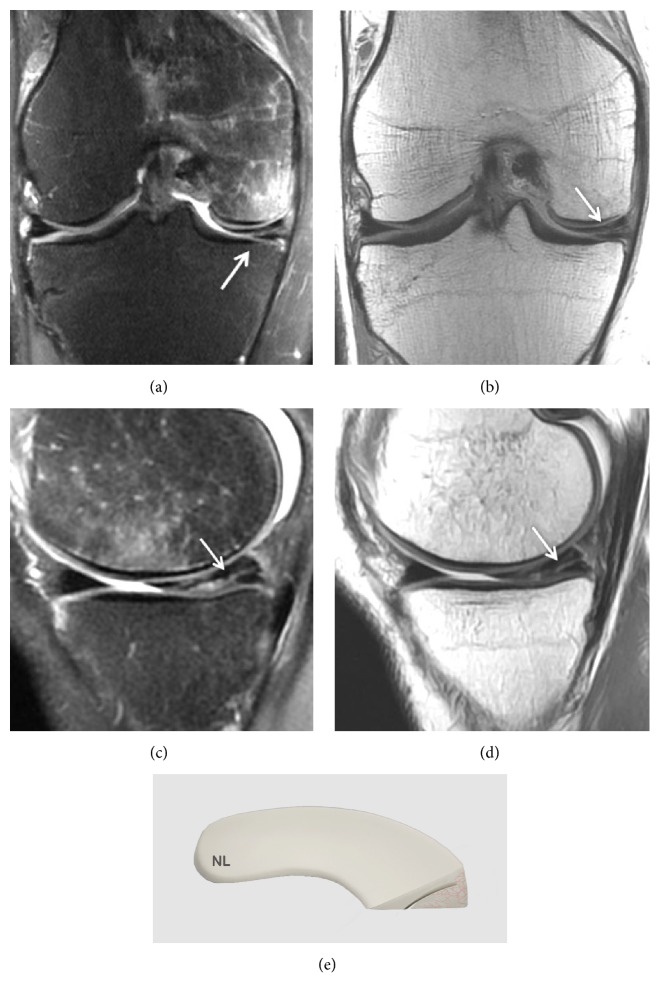
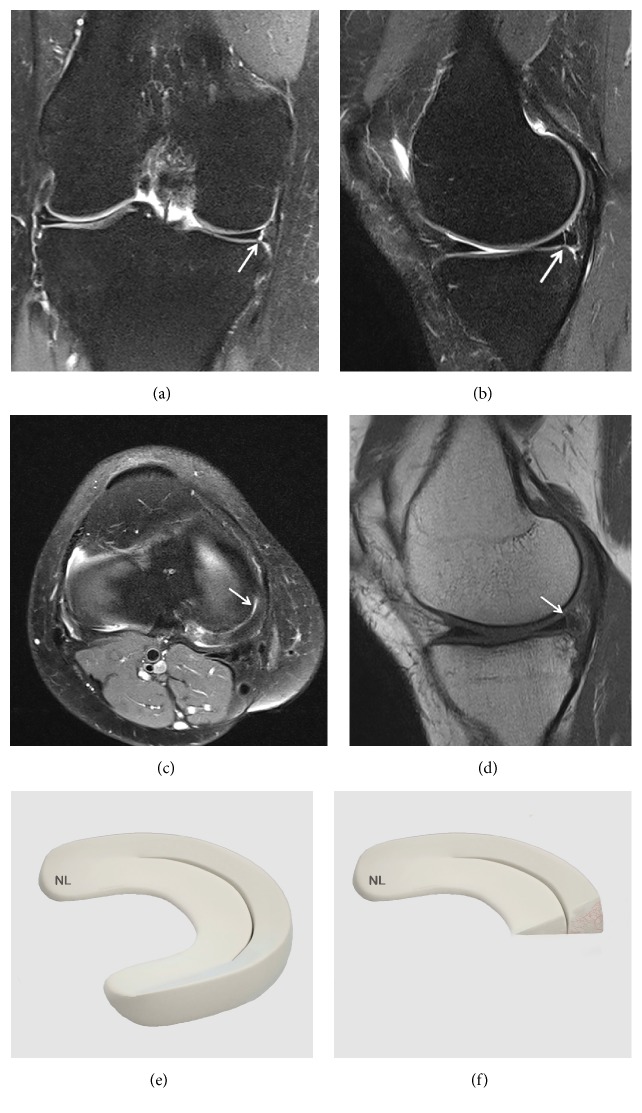
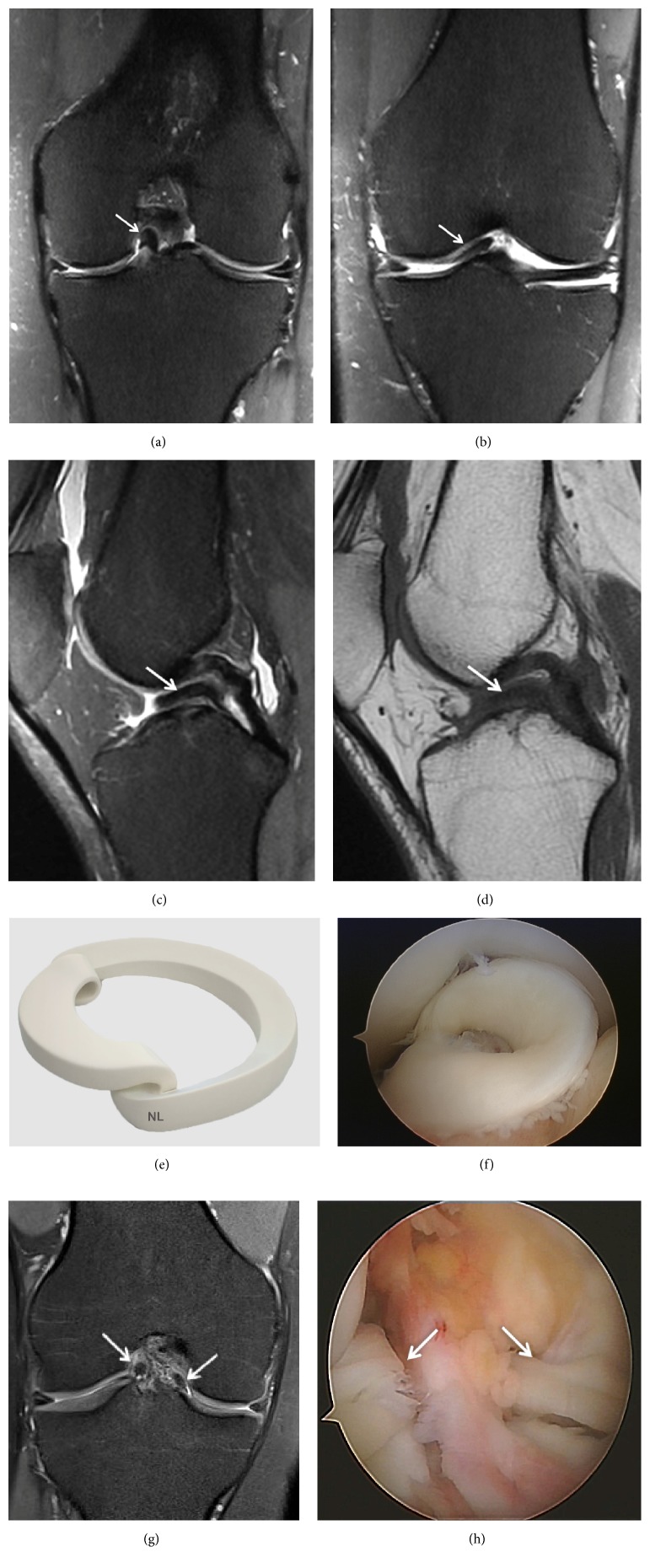
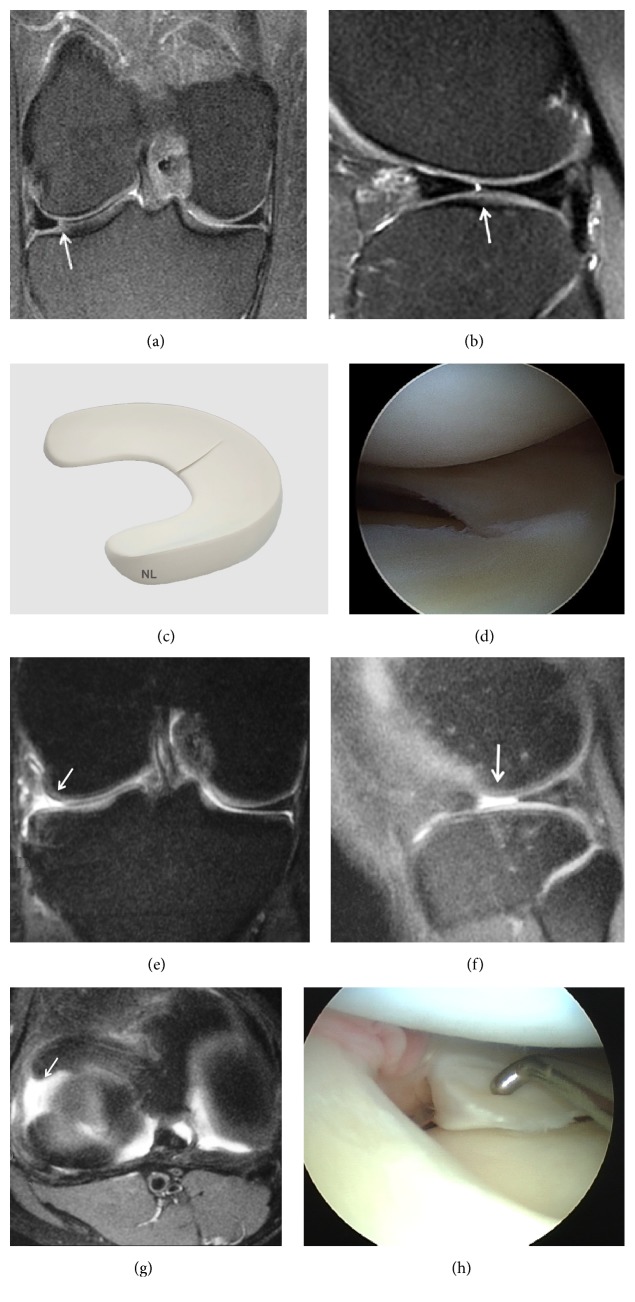
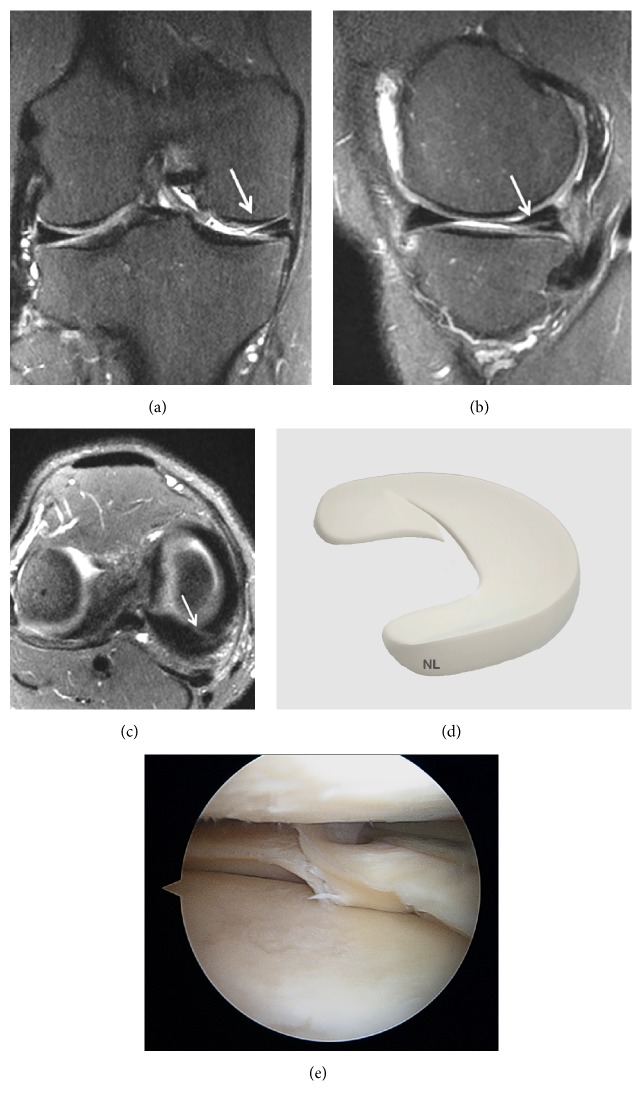
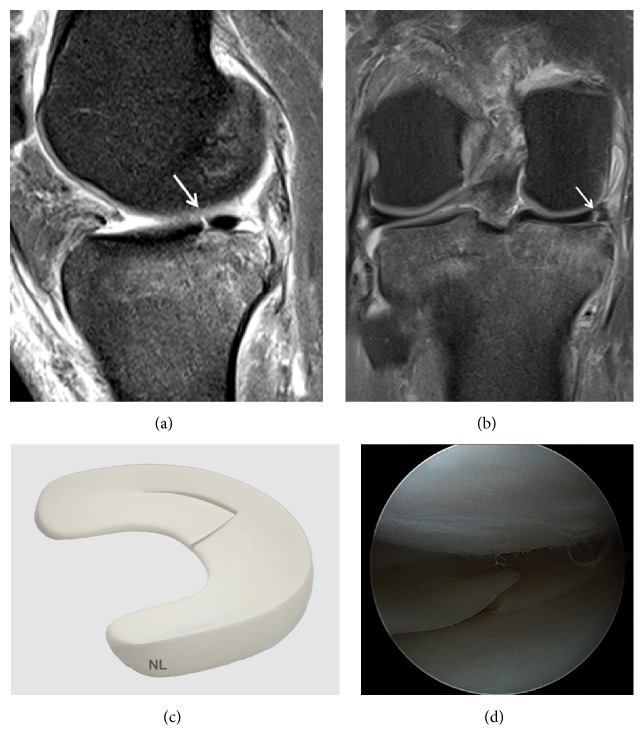
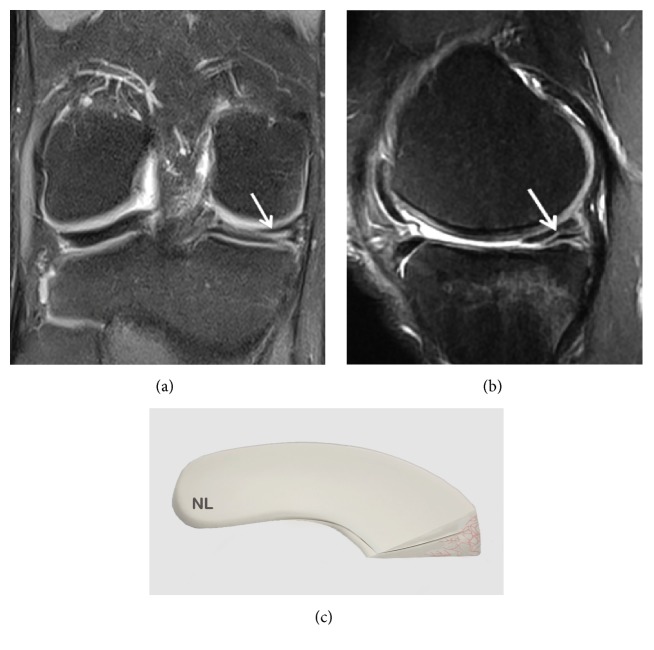
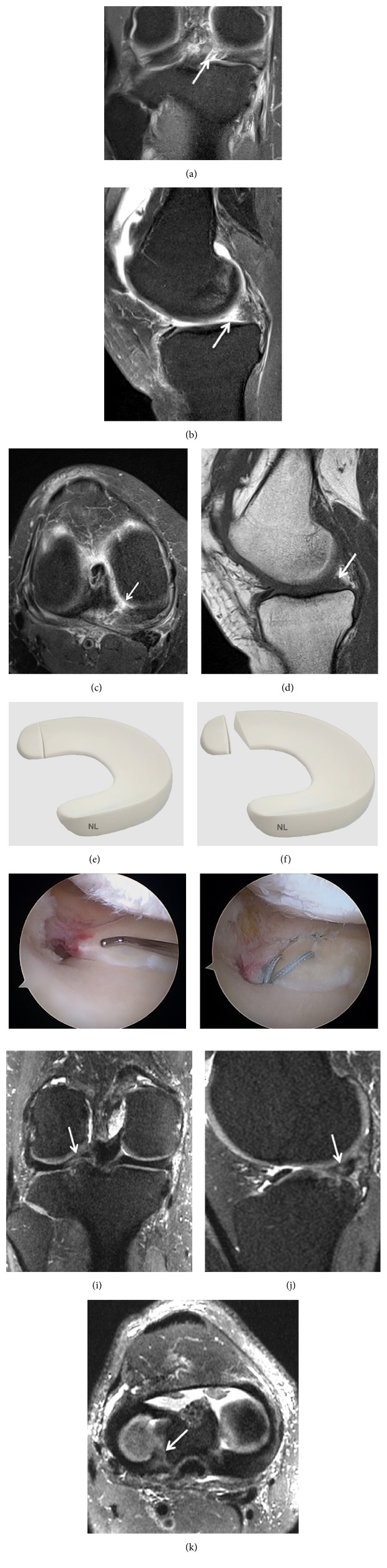
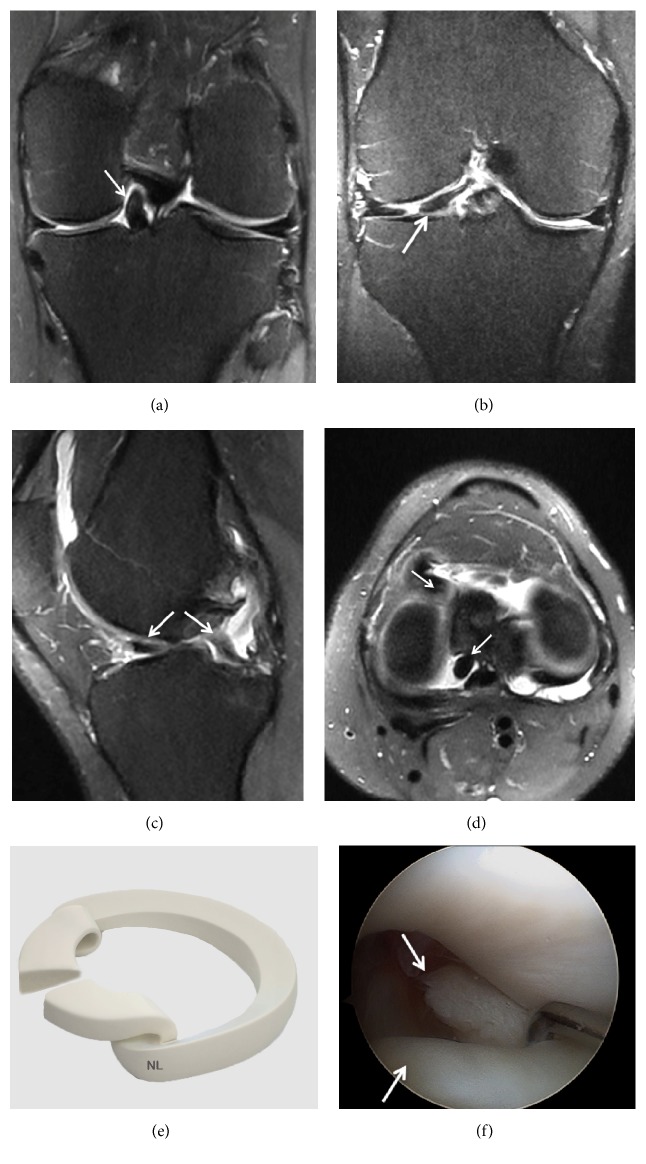
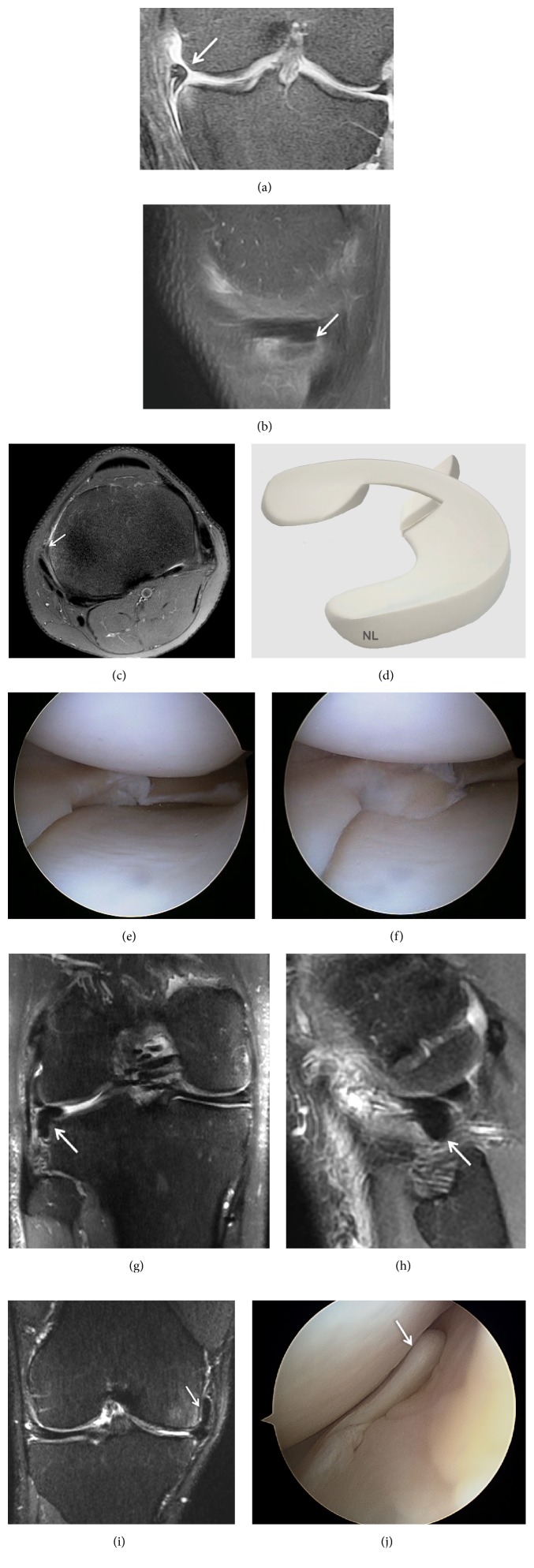
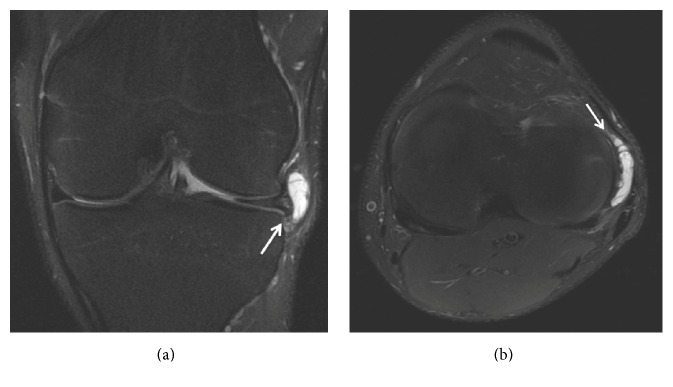
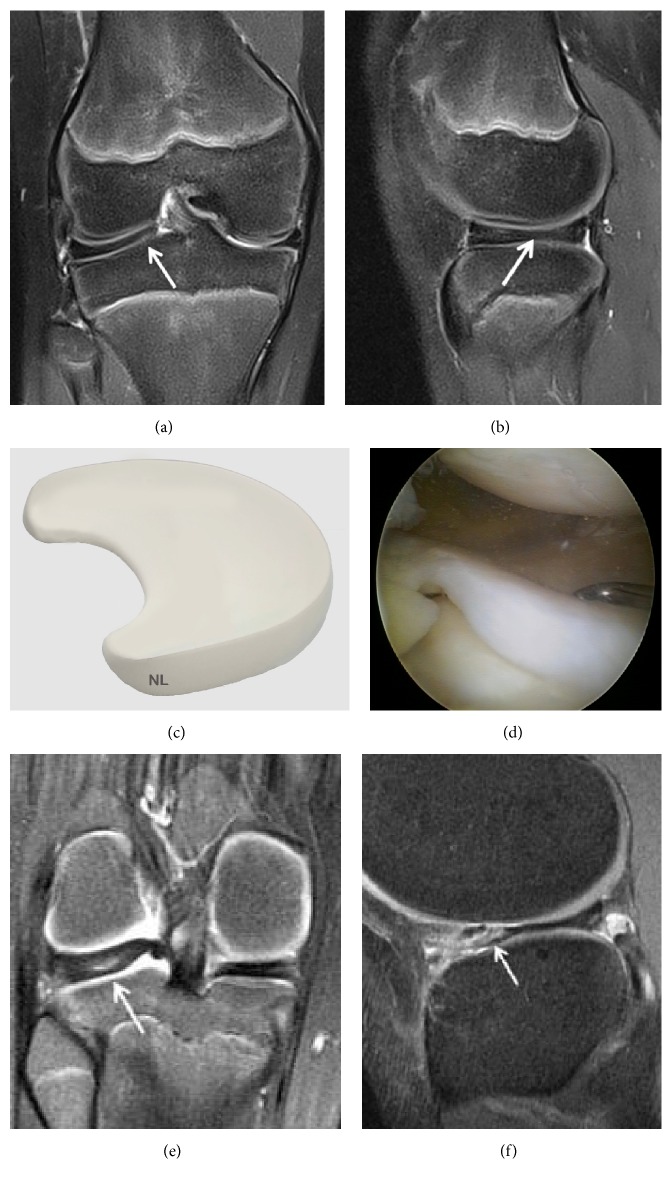
The main objective of this review was to present a synthesis of the current literature in order to provide a useful tool to clinician in radiologic analysis of the meniscus. All anatomical descriptions were clearly illustrated by MRI, arthroscopy, and/or drawings. The value of standard radiography is extremely limited for the assessment of meniscal injuries but may be indicated to obtain a differential diagnosis such as osteoarthritis. Ultrasound is rarely used as a diagnostic tool for meniscal pathologies and its accuracy is operator-dependent. CT arthrography with multiplanar reconstructions can detect meniscus tears that are not visible on MRI. This technique is also useful in case of MRI contraindications, in postoperative assessment of meniscal sutures and the condition of cartilage covering the articular surfaces. MRI is the most accurate and less invasive method for diagnosing meniscal lesions. MRI allows confirming and characterizing the meniscal lesion, the type, the extension, its association with a cyst, the meniscal extrusion, and assessing cartilage and subchondral bone. New 3D-MRI in three dimensions with isotropic resolution allows the creation of multiplanar reformatted images to obtain from an acquisition in one sectional plane reconstructions in other spatial planes. 3D MRI should further improve the diagnosis of meniscal tears.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
