

Efficacy Comparison Between Total Laryngectomy and Nonsurgical Organ-Preservation Modalities in Treatment of Advanced Stage Laryngeal Cancer: A Meta-Analysis
- PMID: 27057837
- PMCID: PMC4998753
- DOI: 10.1097/MD.0000000000003142
Efficacy Comparison Between Total Laryngectomy and Nonsurgical Organ-Preservation Modalities in Treatment of Advanced Stage Laryngeal Cancer: A Meta-Analysis
Abstract
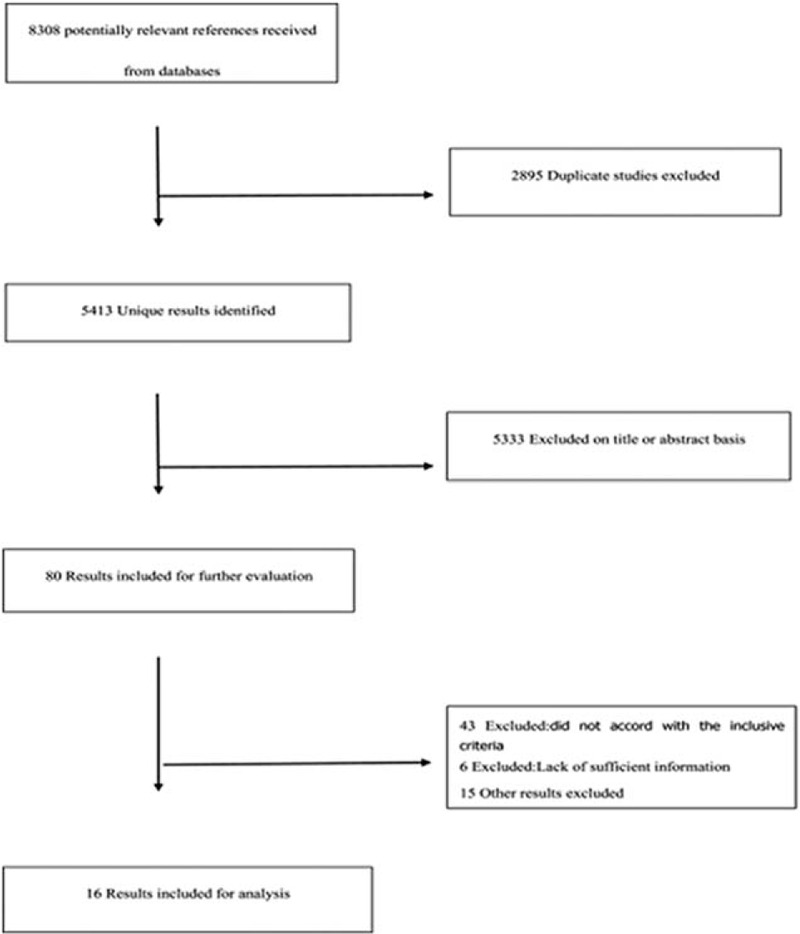
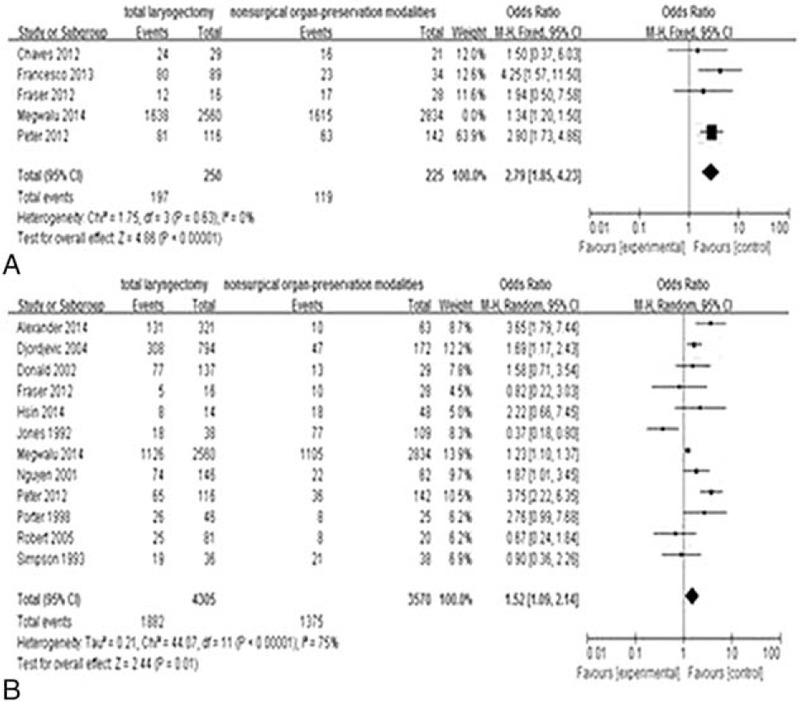
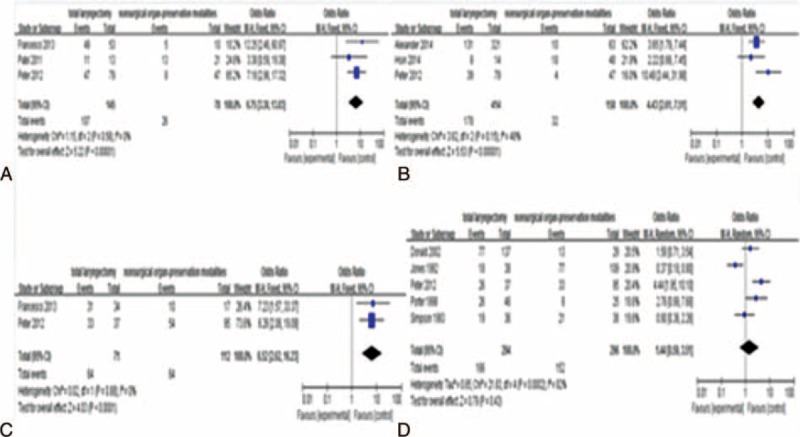
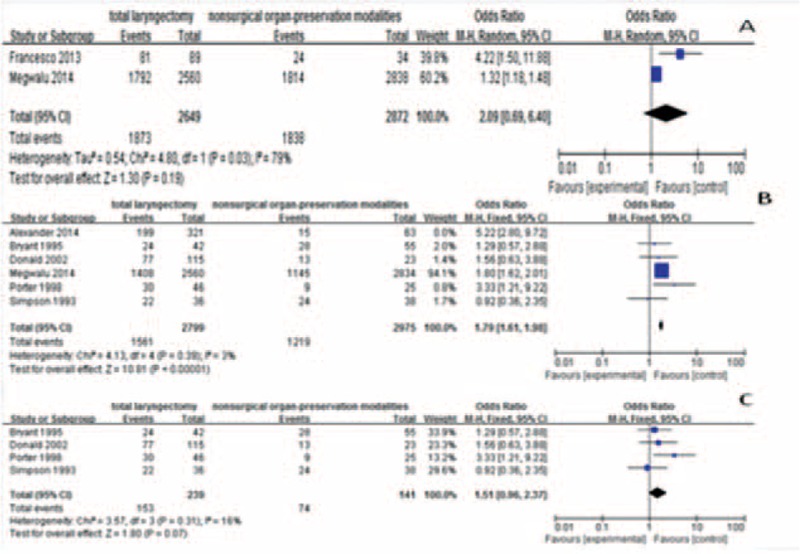
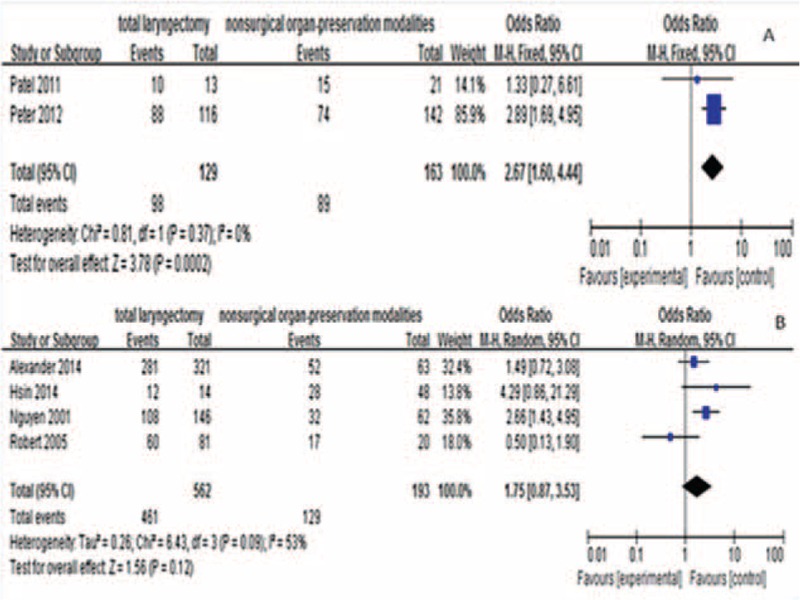
It remains unclear whether the efficacy of nonsurgical organ-preservation modalities (NOP) in the treatment of advanced-stage laryngeal cancer was noninferiority compared with that of total laryngectomy (TL). The objective of this study was to compare the curative effects between TL and NOP in the treatment of advanced-stage laryngeal cancer through a meta-analysis.Clinical studies were retrieved from the electronic databases of PubMed, Embase, Wanfang, and Chinese National Knowledge infrastructure. A meta-analysis was performed to investigate the differences in the curative efficacy of advanced-stage laryngeal cancer between TL and the nonsurgical method. Two reviewers screened all titles and abstracts, and independently assessed all articles. All identified studies were retrospective.Sixteen retrospective studies involving 8308 patients (4478 in the TL group and 3701 in the nonsurgical group) were included in this meta-analysis. The analysis results displayed the advantage of TL for 2-year and 5-year overall survival (OS)(OR 2.79, 95% CI 1.85-4.23 and OR 1.52, 95% CI 1.09-2.14) as well as in 5-year disease-specific survival (DSS)(OR 1.79, 95% CI 1.61-1.98), but no significant difference in 2-year DSS was detected between the 2 groups (OR = 2.09,95% CI0.69-6.40). Additionally, there were no significant differences between TL and NOP for 5-year local control (LC) either (OR = 1.75, 95% CI 0.87-3.53). When we carried out subgroup analyses, the advantage of TL was especially obvious in T4 subgroups, but not in T3 subgroups.This is the first study to compare the curative effects on advanced-stage laryngeal cancer using meta-analytic methodology. Although there was a trend in favor of TL for OS and DSS, there is no clear difference in oncologic outcome between TL and NOP. Therefore, other factors such as tumor T-stage and size, lymph node metastasis, and physical condition are also important indicators for treatment choice.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007. CA Cancer J Clin 2007; 57:43–66. - PubMed
-
- American Cancer Society. Cancer Facts & Figures 2010. Atlanta, GA: American Cancer Society; 2010.
-
- Barnes L, Tse LY, Hunt JL. Barnes L, Eveson J, Reichart P, Sidransky D, et al. Tumours of the hypopharynx, larynx and trachea: introduction. World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours.. Lyon, France: IARC Press; 2005. 111–117.
-
- Mendenhall WM, Werning JW, Hinerman RW, et al. Management of T1-T2 glottic carcinomas. Cancer 2004; 100:1786–1792. - PubMed
-
- Shah JP, Karnell LH, Hoffman HT, et al. Patterns of care for cancer of the larynx in the United States. Arch Otolaryngol Head Neck Surg 1997; 123:475–483. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
