

Effect of hemoadsorption during cardiopulmonary bypass surgery - a blinded, randomized, controlled pilot study using a novel adsorbent
- PMID: 27059056
- PMCID: PMC4826492
- DOI: 10.1186/s13054-016-1270-0
Effect of hemoadsorption during cardiopulmonary bypass surgery - a blinded, randomized, controlled pilot study using a novel adsorbent
Abstract
Background: Cardiopulmonary bypass (CPB) surgery initiates a systemic inflammatory response, which is associated with postoperative morbidity and mortality. Hemoadsorption (HA) of cytokines may suppress inflammatory responses and improve outcomes. We tested a new sorbent used for HA (CytoSorb™; CytoSorbents Europe GmbH, Berlin, Germany) installed in the CPB circuit on changes of pro- and anti-inflammatory cytokines levels, inflammation markers, and differences in patients' perioperative course.
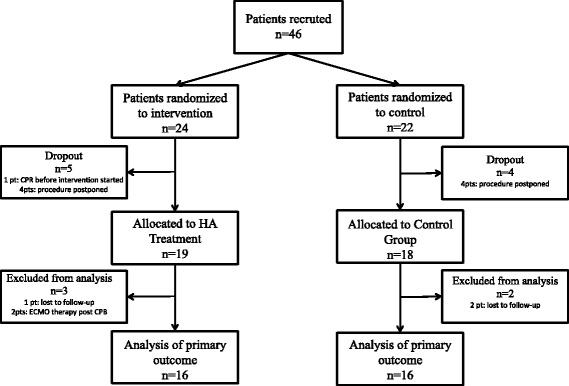
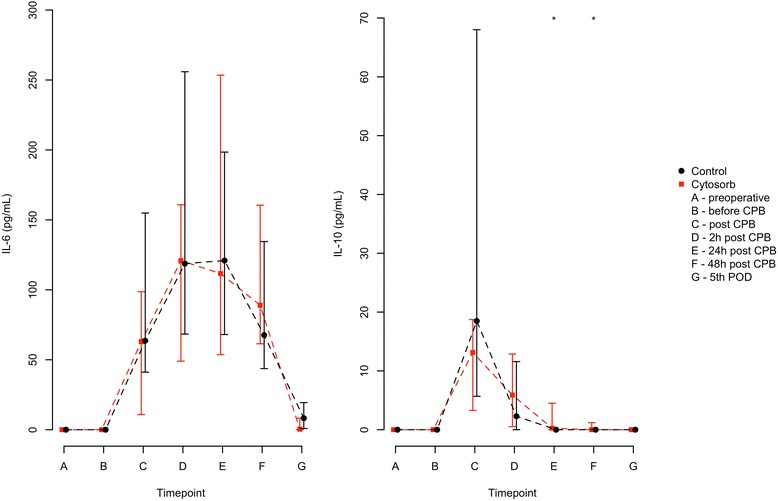
Methods: In this first pilot trial, 37 blinded patients were undergoing elective CPB surgery at the Medical University of Vienna and were randomly assigned to HA (n = 19) or control group (n = 18). The primary outcome was differences of cytokine levels (IL-1β, IL-6, IL-18, TNF-α, and IL-10) within the first five postoperative days. We also analyzed whether we can observe any differences in ex vivo lipopolysaccharide (LPS)-induced TNF-α production, a reduction of high-mobility box group 1 (HMGB1), or other inflammatory markers. Additionally, measurements for fluid components, blood products, catecholamine treatment, bioelectrical impedance analysis (BIA), and 30-day mortality were analyzed.
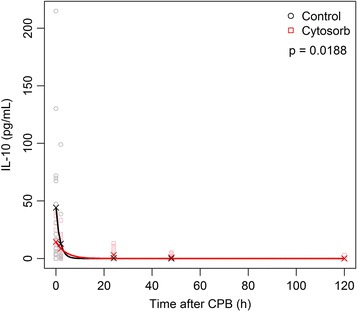
Results: We did not find differences in our primary outcome immediately following the HA treatment, although we observed differences for IL-10 24 hours after CPB (HA: median 0.3, interquartile range (IQR) 0-4.5; control: not traceable, P = 0.0347) and 48 hours after CPB (median 0, IQR 0-1.2 versus not traceable, P = 0.0185). We did not find any differences for IL-6 between both groups, and other cytokines were rarely expressed. We found differences in pretreatment levels of HMGB1 (HA: median 0, IQR 0-28.1; control: median 48.6, IQR 12.7-597.3, P = 0.02083) but no significant changes to post-treatment levels. No differences in inflammatory markers, fluid administration, blood substitution, catecholamines, BIA, or 30-day mortality were found.
Conclusions: We did not find any reduction of the pro-inflammatory response in our patients and therefore no changes in their perioperative course. However, IL-10 showed a longer-lasting anti-inflammatory effect. The clinical impact of prolonged IL-10 needs further evaluation. We also observed strong inter-individual differences in cytokine levels; therefore, patients with an exaggerated inflammatory response to CPB need to be identified. The implementation of HA during CPB was feasible.
Trial registration: ClinicalTrials.gov: NCT01879176, registration date: June 7, 2013.
Keywords: Cardiac surgery; Cardiopulmonary bypass; CytoSorb; Cytokine storm; Cytokines; Hemadsorption; High-mobility box group 1; Inflammation; Interleukin.
Figures
References
-
- Tomic V, Russwurm S, Moller E, Claus RA, Blaess M, Brunkhorst F, et al. Transcriptomic and proteomic patterns of systemic inflammation in on-pump and off-pump coronary artery bypass grafting. Circulation. 2005;112:2912–2920. - PubMed
-
- Diegeler A, Doll N, Rauch T, Haberer D, Walther T, Falk V, et al. Humoral immune response during coronary artery bypass grafting: A comparison of limited approach, “off-pump” technique, and conventional cardiopulmonary bypass. Circulation. 2000;102(19 Suppl 3):III95–III100. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
