

Impact of strategies to reduce polypharmacy on clinically relevant endpoints: a systematic review and meta-analysis
- PMID: 27059768
- PMCID: PMC4972170
- DOI: 10.1111/bcp.12959
Impact of strategies to reduce polypharmacy on clinically relevant endpoints: a systematic review and meta-analysis
Abstract
Aim: The aim of the present study was to explore the impact of strategies to reduce polypharmacy on mortality, hospitalization and change in number of drugs.
Methods: Systematic review and meta-analysis: a systematic literature search targeting patients ≥65 years with polypharmacy (≥4 drugs), focusing on patient-relevant outcome measures, was conducted. We included controlled studies aiming to reduce polypharmacy. Two reviewers independently assessed studies for eligibility, extracted data and evaluated study quality.
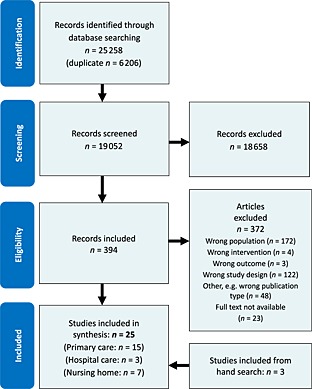
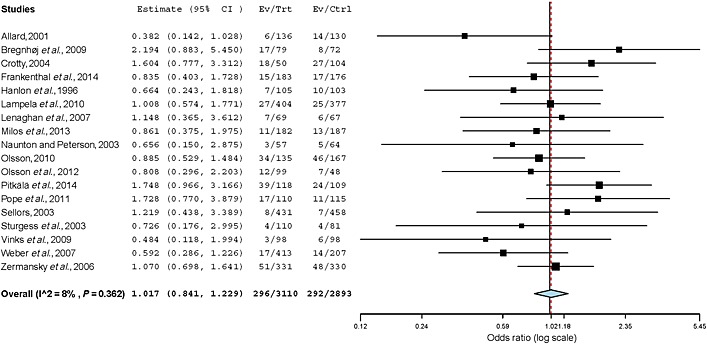
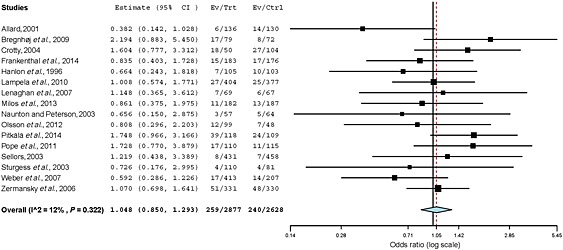
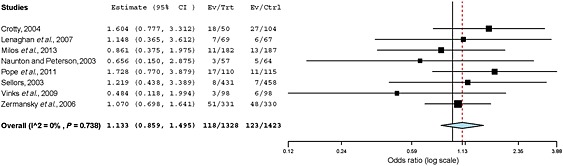
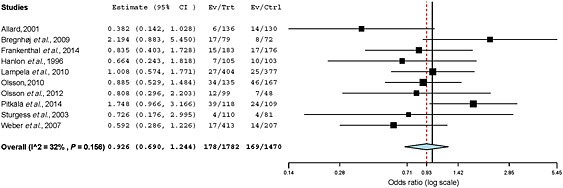
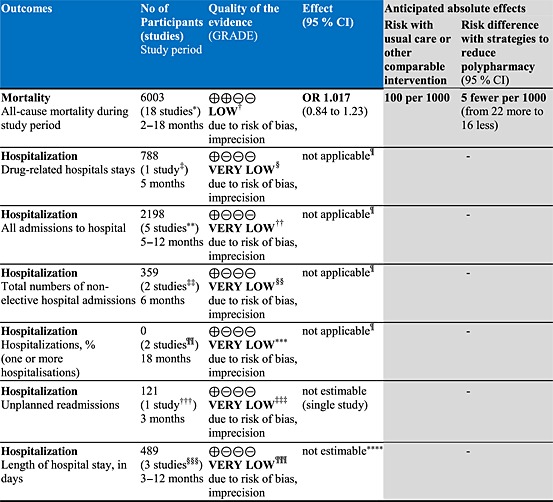
Results: Twenty-five studies, including 10 980 participants, were included, comprising 21 randomized controlled trials and four nonrandomized controlled trials. The majority of the included studies aimed at improving quality or the appropriateness of prescribing by eliminating inappropriate and non-evidence-based drugs. These strategies to reduce polypharmacy had no effect on all-cause mortality (odds ratio 1.02; 95% confidence interval 0.84, 1.23). Only single studies found improvements, in terms of reducing the number of hospital admissions, in favour of the intervention group. At baseline, patients were taking, on average, 7.4 drugs in both the intervention and the control groups. At follow-up, the weighted mean number of drugs was reduced (-0.2) in the intervention group but increased (+0.2) in controls.
Conclusions: There is no convincing evidence that the strategies assessed in the present review are effective in reducing polypharmacy or have an impact on clinically relevant endpoints. Interventions are complex; it is still unclear how best to organize and implement them to achieve a reduction in inappropriate polypharmacy. There is therefore a need to develop more effective strategies to reduce inappropriate polypharmacy and to test them in large, pragmatic randomized controlled trials on effectiveness and feasibility.
Keywords: aged; hospitalisation; medication therapy management; meta-analysis; mortality; polypharmacy.
© 2016 The British Pharmacological Society.
Figures
Comment in
-
Endpoints in strategies to reduce polypharmacy.Br J Clin Pharmacol. 2017 Feb;83(2):432-433. doi: 10.1111/bcp.13122. Epub 2016 Sep 29. Br J Clin Pharmacol. 2017. PMID: 27680503 Free PMC article. No abstract available.
-
Reply to 'Endpoints in strategies to reduce polypharmacy'.Br J Clin Pharmacol. 2017 Feb;83(2):434. doi: 10.1111/bcp.13125. Epub 2016 Oct 4. Br J Clin Pharmacol. 2017. PMID: 27704600 Free PMC article. No abstract available.
References
-
- Corsonello A, Pedone C, Incalzi RA. Age‐related pharmacokinetic and pharmacodynamic changes and related risk of adverse drug reactions. Curr Med Chem 2010; 17: 571–84. - PubMed
-
- Slabaugh SL, Maio V, Templin M, Abouzaid S. Prevalence and risk of polypharmacy among the elderly in an outpatient setting: a retrospective cohort study in the Emilia‐Romagna region, Italy. Drugs Aging 2010; 27: 1019–28. - PubMed
-
- Rohrer JE, Garrison G, Oberhelman SA, Meunier MR. Epidemiology of polypharmacy among family medicine patients at hospital discharge. J Prim Care Community Health 2013; 4: 101–5. - PubMed
-
- Fialova D, Topinkova E, Gambassi G, Finne‐Soveri H, Jonsson PV, Carpenter I, et al. Potentially inappropriate medication use among elderly home care patients in Europe. JAMA 2005; 293: 1348–58. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
