

A Quantitative Analysis of Subclonal and Clonal Gene Mutations before and after Therapy in Chronic Lymphocytic Leukemia
- PMID: 27060156
- PMCID: PMC5010528
- DOI: 10.1158/1078-0432.CCR-15-3103
A Quantitative Analysis of Subclonal and Clonal Gene Mutations before and after Therapy in Chronic Lymphocytic Leukemia
Abstract
Purpose: Chronic lymphocytic leukemia (CLL)-associated gene mutations that influence CLL cell fitness and chemotherapy resistance should increase in clonal representation when measured before therapy and at relapse.
Experimental design: To uncover mutations associated with CLL relapse, we have performed whole-exome sequencing in a discovery cohort of 61 relapsed CLL patients identifying 86 recurrently mutated genes. The variant allele fractions (VAF) of 19 genes with mutations in ≥3 of 61 cases were measured in 53 paired pre- and posttreatment CLL samples sorted to purity using panel-based deep resequencing or by droplet digital PCR.
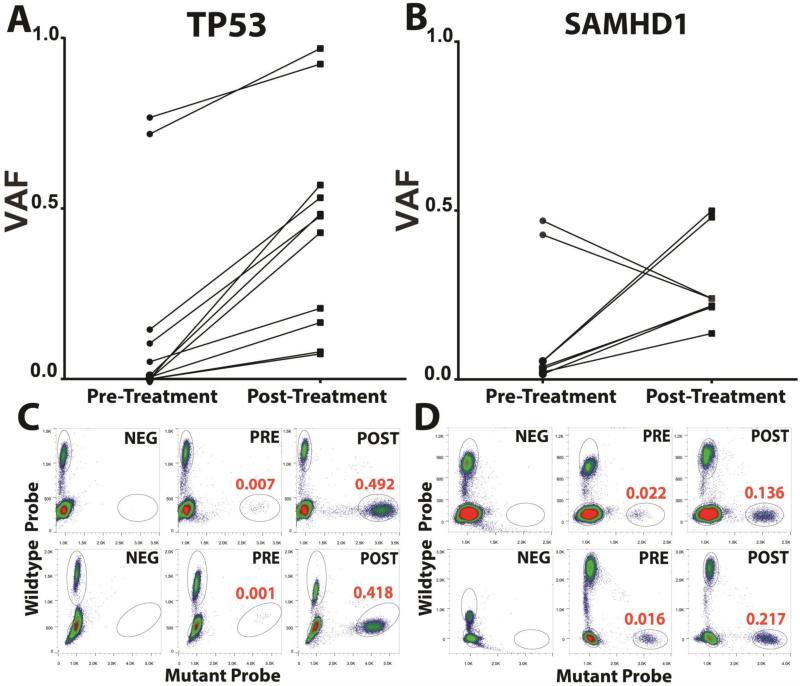
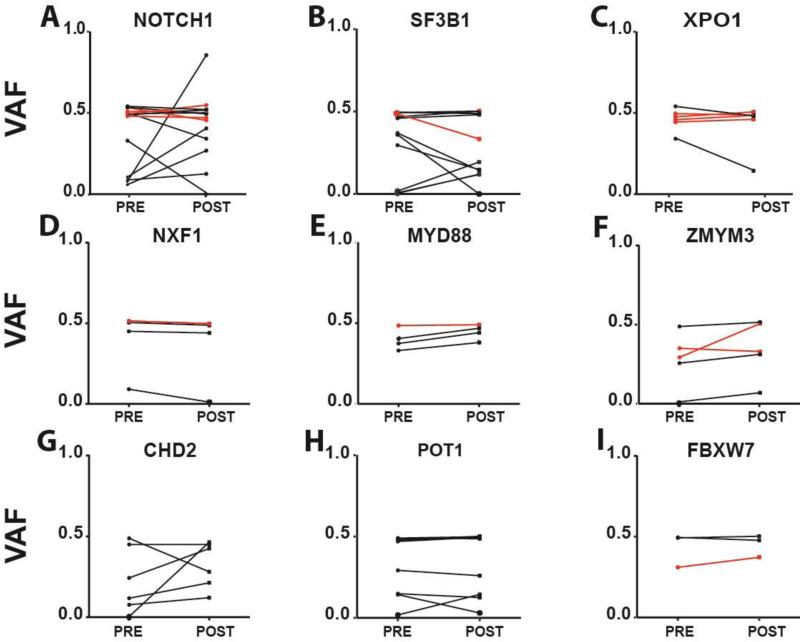
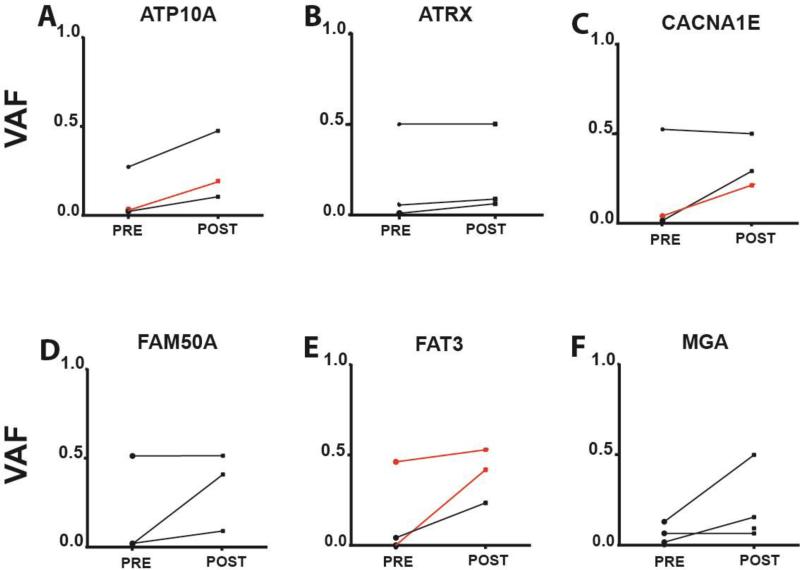
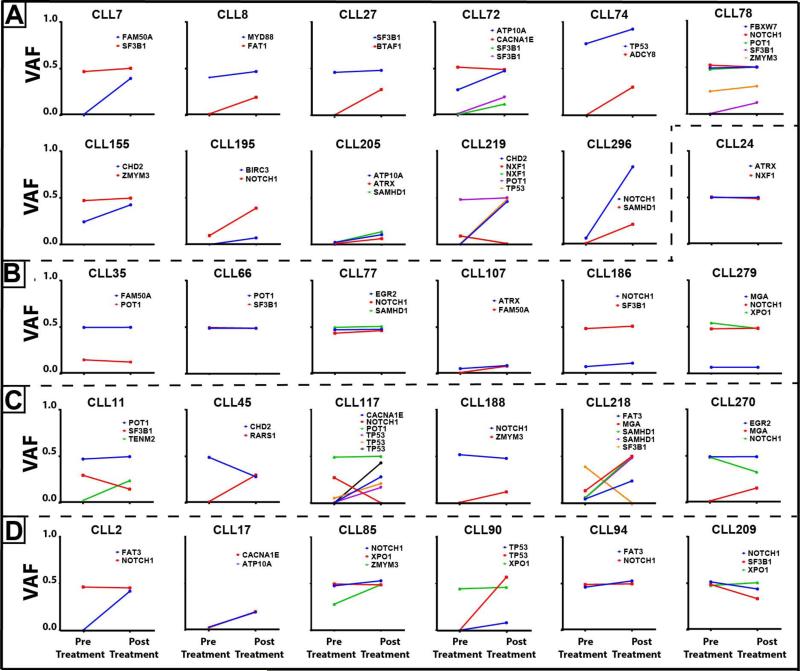
Results: We identify mutations in TP53 as the dominant subclonal gene driver of relapsed CLL often demonstrating substantial increases in VAFs. Subclonal mutations in SAMHD1 also recurrently demonstrated increased VAFs at relapse. Mutations in ATP10A, FAT3, FAM50A, and MGA, although infrequent, demonstrated enrichment in ≥2 cases each. In contrast, mutations in NOTCH1, SF3B1, POT1, FBXW7, MYD88, NXF1, XPO1, ZMYM3, or CHD2 were predominantly already clonal prior to therapy indicative of a pretreatment pathogenetic driver role in CLL. Quantitative analyses of clonal dynamics uncover rising, stable, and falling clones and subclones without clear evidence that gene mutations other than in TP53 and possibly SAMHD1 are frequently selected for at CLL relapse.
Conclusions: Data in aggregate support a provisional categorization of CLL-associated recurrently mutated genes into three classes (i) often subclonal before therapy and strongly enriched after therapy, or, (ii) mostly clonal before therapy or without further enrichments at relapse, or, (iii) subclonal before and after therapy and enriching only in sporadic cases. Clin Cancer Res; 22(17); 4525-35. ©2016 AACR.
©2016 American Association for Cancer Research.
Figures
References
-
- Zenz T, Mertens D, Kuppers R, Dohner H, Stilgenbauer S. From pathogenesis to treatment of chronic lymphocytic leukaemia. Nat Rev Cancer. 2010;10:37–50. - PubMed
-
- Strefford JC. The genomic landscape of chronic lymphocytic leukaemia: biological and clinical implications. Br J Haematol. 2014 - PubMed
-
- Dohner H, Stilgenbauer S, Benner A, Leupolt E, Krober A, Bullinger L, et al. Genomic aberrations and survival in chronic lymphocytic leukemia. N Engl J Med. 2000;343:1910–6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
