

Nonalcoholic Fatty Liver Disease: Lipids and Insulin Resistance
- PMID: 27063267
- PMCID: PMC4830921
- DOI: 10.1016/j.cld.2015.10.007
Nonalcoholic Fatty Liver Disease: Lipids and Insulin Resistance
Abstract
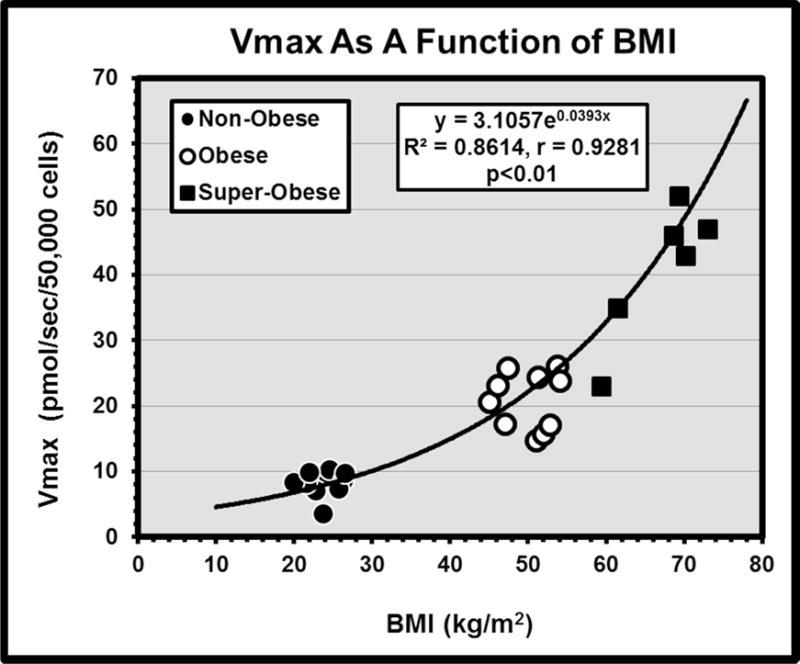
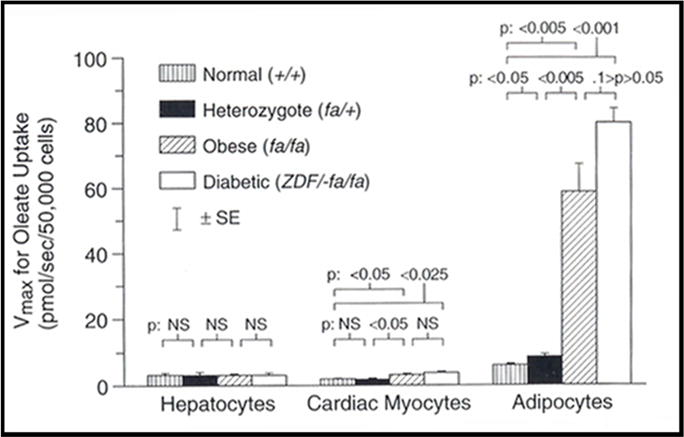
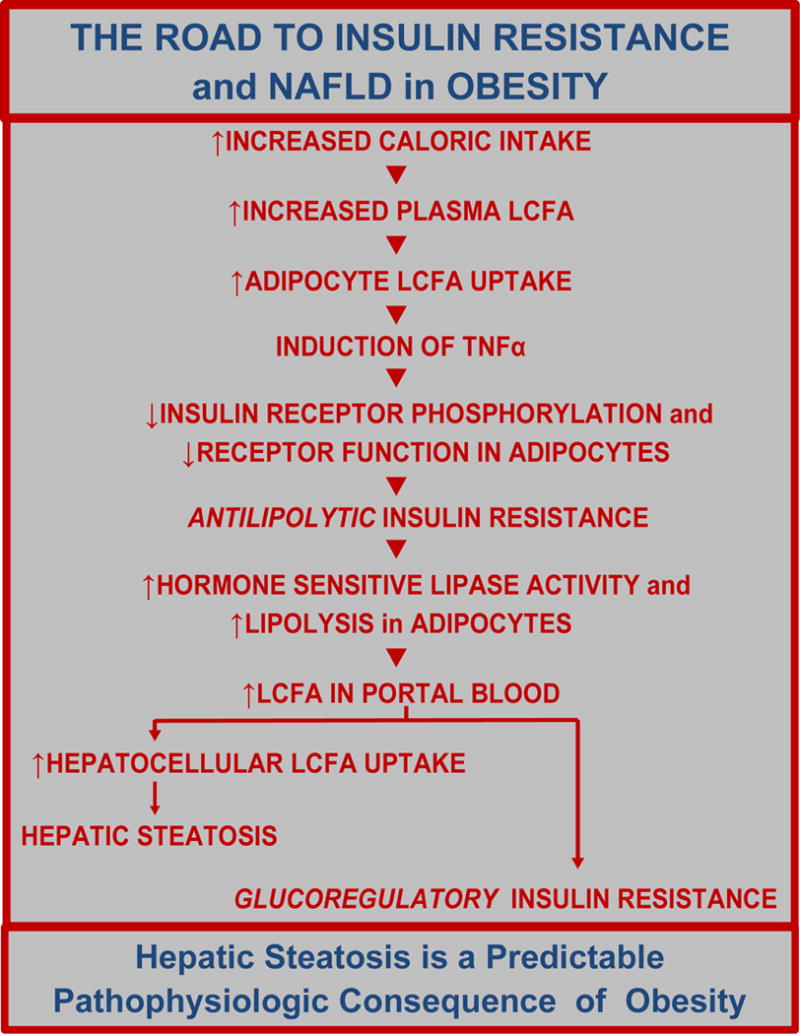
Obesity and its major comorbidities, including type 2 diabetes mellitus, nonalcoholic fatty liver disease (NAFLD), obesity cardiomyopathy, and certain cancers, have caused life expectancy in the United States to decline in recent years. Obesity is the increased accumulation of triglycerides (TG), which are synthesized from glycerol and long-chain fatty acids (LCFA) throughout the body. LCFA enter adipocytes, hepatocytes, and cardiomyocytes via specific, facilitated transport processes. Metabolism of increased cellular TG content in obesity may lead to comorbidities such as NAFLD and cardiomyopathy. Better understanding of LCFA transport processes may lead to successful treatment of obesity and NAFLD.
Keywords: Facilitated transport; Leptin; Lipotoxicity; Spexin; Weight regain.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohepatitis: Mayo clinic experiences with a hitherto unnamed disease. Mayo Clin Proc. 1980;55:434–438. - PubMed
-
- Diehl AM, Goodman Z, Ishak KG. Alcohol-like liver disease in non-alcoholics. Gastroenterol. 1988;95:1056–1062. - PubMed
-
- Clain DJ, Lefkowitch JH. Fatty liver disease in morbid obesity. Gastroenterol Clin N Amer. 1987;16:239–252. - PubMed
-
- Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, Charlton M, Sanyal AJ, American Gastroenterological Association; American Association for the Study of Liver Diseases; American College of Gastroenterology The diagnosis and management of nonalcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroentl. 2012 Jun;142(7):1592–1609. doi: 10.1053/j.gastro.2012.04.001. - DOI - PubMed
-
- Burt AD, Lackner C, Tiniakos DG. Diagnosis and assessment of NAFLD: definitions and histopathological classification. Semin Liv Dis. 2015 Aug;35(3):207–220. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
