

Postoperative Mortality after Liver Resection for Perihilar Cholangiocarcinoma: Development of a Risk Score and Importance of Biliary Drainage of the Future Liver Remnant
- PMID: 27063572
- PMCID: PMC4961586
- DOI: 10.1016/j.jamcollsurg.2016.03.035
Postoperative Mortality after Liver Resection for Perihilar Cholangiocarcinoma: Development of a Risk Score and Importance of Biliary Drainage of the Future Liver Remnant
Abstract
Background: Liver surgery for perihilar cholangiocarcinoma (PHC) is associated with postoperative mortality ranging from 5% to 18%. The aim of this study was to develop a preoperative risk score for postoperative mortality after liver resection for PHC, and to assess the effect of biliary drainage of the future liver remnant (FLR).
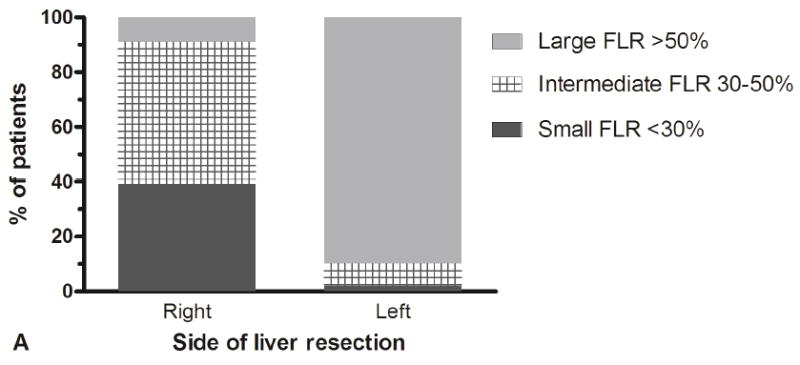
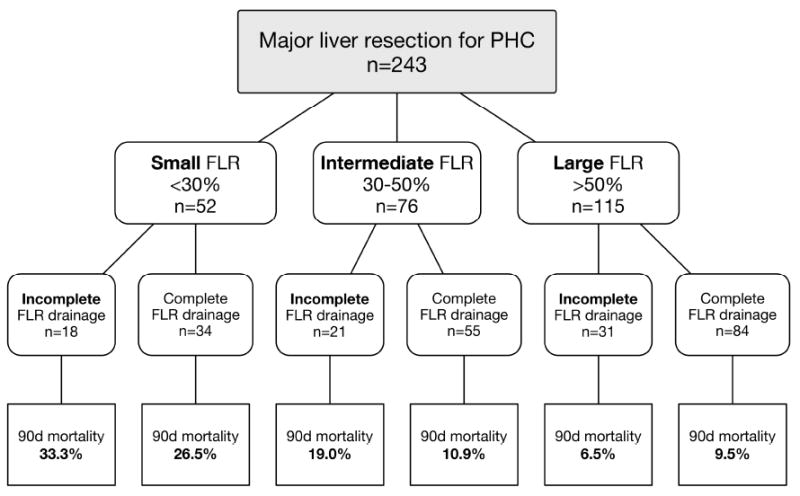
Study design: A consecutive series of 287 patients submitted to major liver resection for presumed PHC between 1997 and 2014 at 2 Western centers was analyzed; 228 patients (79%) underwent preoperative drainage for jaundice. Future liver remnant volumes were calculated with CT volumetry and completeness of FLR drainage was assessed on imaging. Logistic regression was used to develop a mortality risk score.
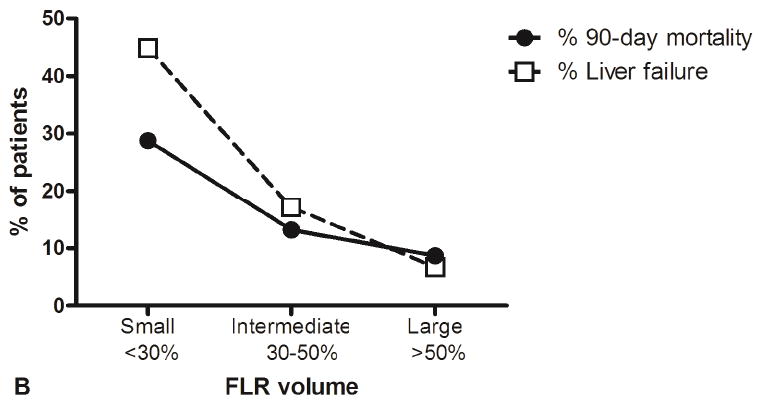
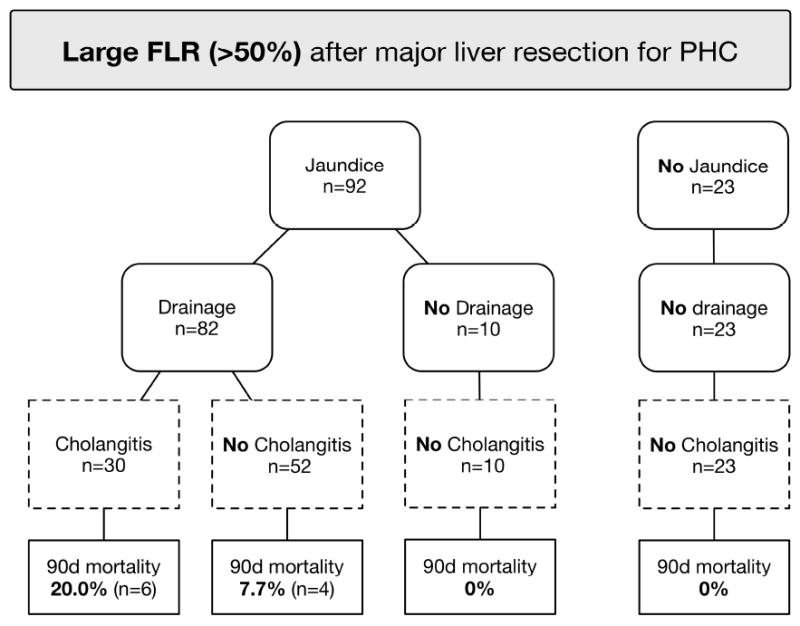
Results: Postoperative mortality at 90 days was 14% and was independently predicted by age (odds ratio [OR] per 10 years = 2.1), preoperative cholangitis (OR = 4.1), FLR volume <30% (OR = 2.9), portal vein reconstruction (OR = 2.3), and incomplete FLR drainage in patients with FLR volume <50% (OR = 2.8). The risk score showed good discrimination (area under the curve = 0.75 after bootstrap validation) and ranking patients in tertiles identified 3 (ie low, intermediate, and high) risk subgroups with predicted mortalities of 2%, 11%, and 37%. No postoperative mortality was observed in 33 undrained patients with FLR volumes >50%, including 10 jaundiced patients (median bilirubin level 11 mg/dL).
Conclusions: The mortality risk score for patients with resectable PHC can be used for patient counseling and identification of modifiable risk factors, which include FLR volume, FLR drainage status, and preoperative cholangitis. We found no evidence to support preoperative biliary drainage in patients with an FLR volume >50%.
Copyright © 2016 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. - PubMed
-
- Ito F, Agni R, Rettammel RJ, et al. Resection of hilar cholangiocarcinoma: concomitant liver resection decreases hepatic recurrence. Ann Surg. 2008 Aug;248(2):273–9. - PubMed
-
- Nagino M, Ebata T, Yokoyama Y, et al. Evolution of surgical treatment for perihilar cholangiocarcinoma: a single-center 34-year review of 574 consecutive resections. Ann Surg. 2013 Jul;258(1):129–40. - PubMed
-
- Nuzzo G, Giuliante F, Ardito F, et al. Improvement in perioperative and long-term outcome after surgical treatment of hilar cholangiocarcinoma: results of an Italian multicenter analysis of 440 patients. Arch Surg. 2012 Jan;147(1):26–34. - PubMed
-
- Farges O, Regimbeau JM, Fuks D, et al. Multicentre European study of preoperative biliary drainage for hilar cholangiocarcinoma. Br J Surg. 2013 Jan;100(2):274–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
