

Lung Circulation
- PMID: 27065170
- PMCID: PMC7432532
- DOI: 10.1002/cphy.c140049
Lung Circulation
Abstract
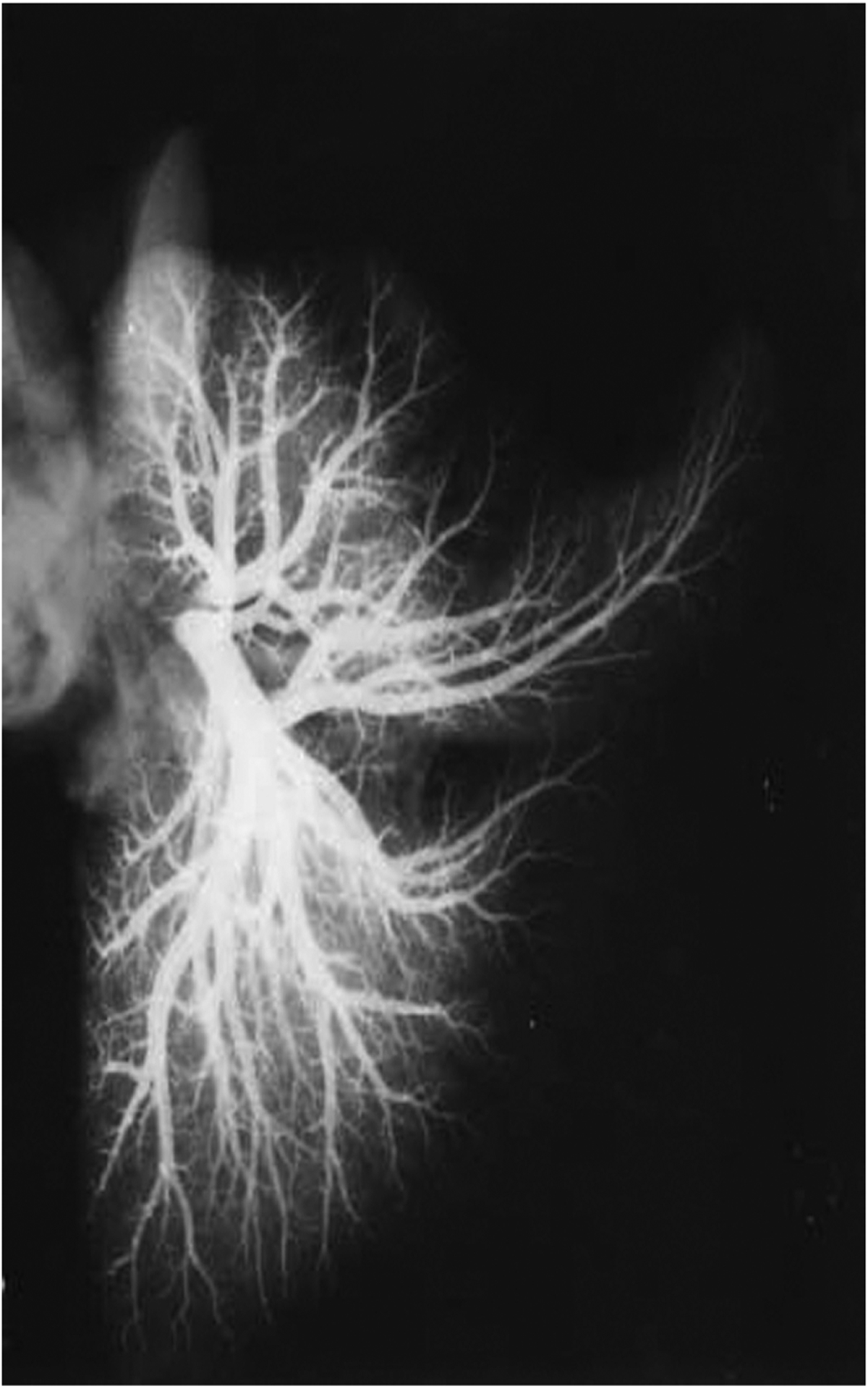
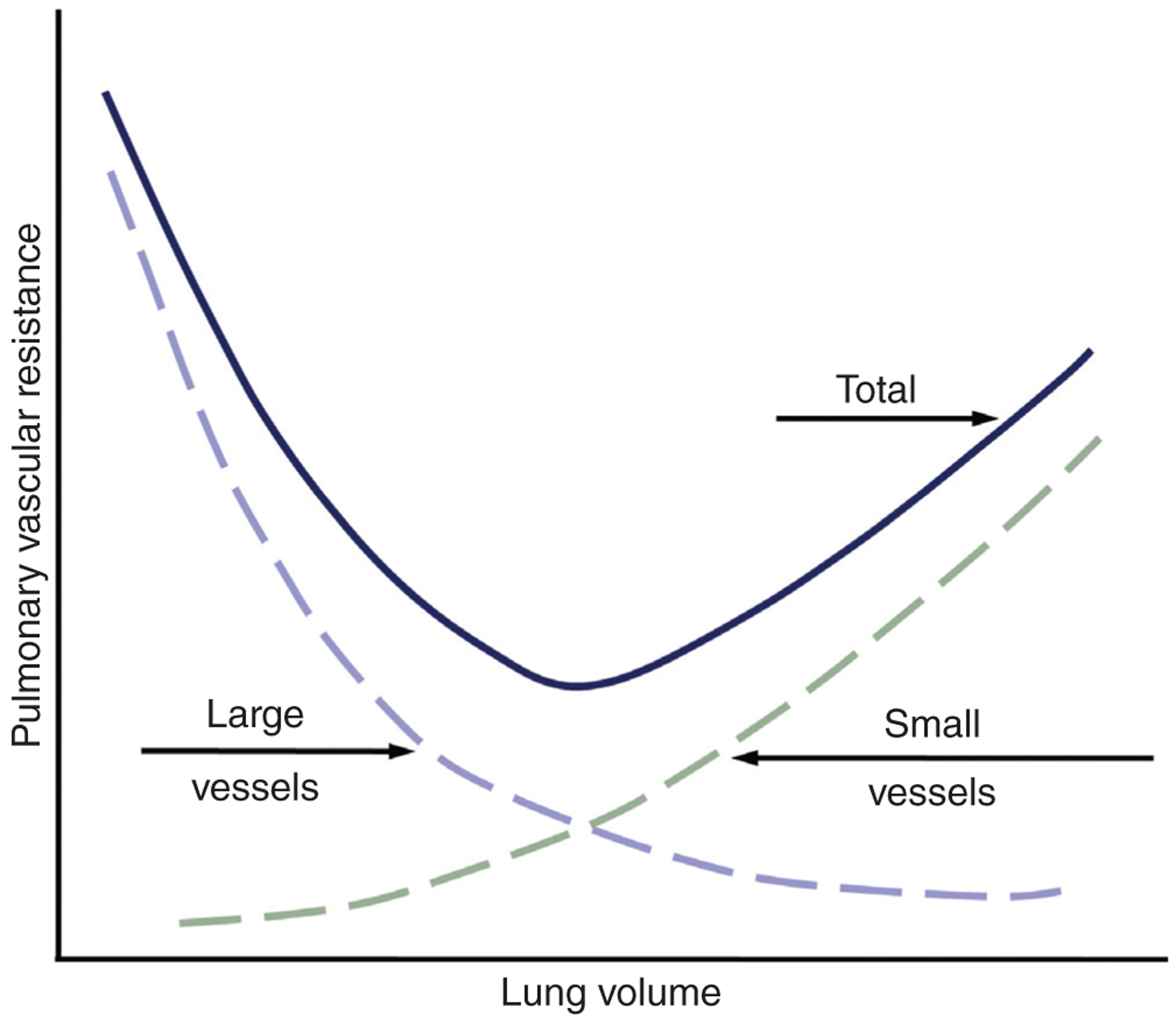
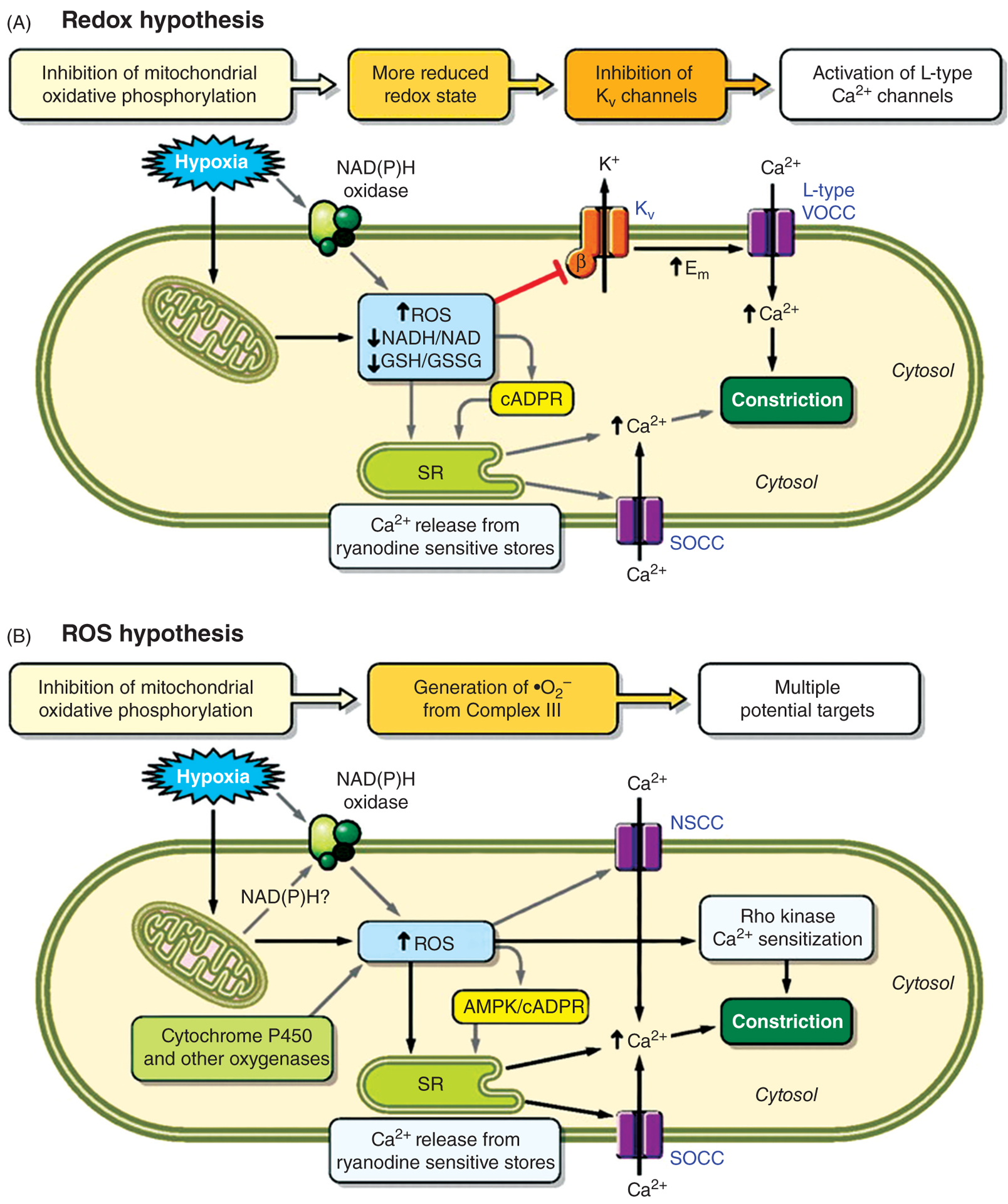
The circulation of the lung is unique both in volume and function. For example, it is the only organ with two circulations: the pulmonary circulation, the main function of which is gas exchange, and the bronchial circulation, a systemic vascular supply that provides oxygenated blood to the walls of the conducting airways, pulmonary arteries and veins. The pulmonary circulation accommodates the entire cardiac output, maintaining high blood flow at low intravascular arterial pressure. As compared with the systemic circulation, pulmonary arteries have thinner walls with much less vascular smooth muscle and a relative lack of basal tone. Factors controlling pulmonary blood flow include vascular structure, gravity, mechanical effects of breathing, and the influence of neural and humoral factors. Pulmonary vascular tone is also altered by hypoxia, which causes pulmonary vasoconstriction. If the hypoxic stimulus persists for a prolonged period, contraction is accompanied by remodeling of the vasculature, resulting in pulmonary hypertension. In addition, genetic and environmental factors can also confer susceptibility to development of pulmonary hypertension. Under normal conditions, the endothelium forms a tight barrier, actively regulating interstitial fluid homeostasis. Infection and inflammation compromise normal barrier homeostasis, resulting in increased permeability and edema formation. This article focuses on reviewing the basics of the lung circulation (pulmonary and bronchial), normal development and transition at birth and vasoregulation. Mechanisms contributing to pathological conditions in the pulmonary circulation, in particular when barrier function is disrupted and during development of pulmonary hypertension, will also be discussed.
Copyright © 2016 John Wiley & Sons, Inc.
Figures






References
-
- Abe K, Shimokawa H, Morikawa K, Uwatoku T, Oi K, Matsumoto Y, Hattori T, Nakashima Y, Kaibuchi K, Sueishi K, Takeshit A. Long-term treatment with a Rho-kinase inhibitor improves monocrotaline-induced fatal pulmonary hypertension in rats. Circ Res 94: 385–393, 2004. - PubMed
-
- Abe K, Toba M, Alzoubi A, Ito M, Fagan KA, Cool CD, Voelkel NF, McMurtry IF, Oka M. Formation of plexiform lesions in experimental severe pulmonary arterial hypertension. Circulation 121: 2747–2754, 2010. - PubMed
-
- Abe T, Arakawa Y, Rajasekaran AK, Yu TH, Wada O. Interaction of atrial natriuretic peptide with its receptors in bovine lung membranes. J Biol Chem 270: 7672–7678, 1995. - PubMed
-
- Abman SH, Accurso FJ. Acute effects of partial compression of ductus arteriosus on fetal pulmonary circulation. Am J Physiol 257: H626–H634, 1989. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
