

Cytoreductive Surgery and Peritonectomy Procedures
- PMID: 27065704
- PMCID: PMC4818624
- DOI: 10.1007/s13193-016-0505-5
Cytoreductive Surgery and Peritonectomy Procedures
Abstract
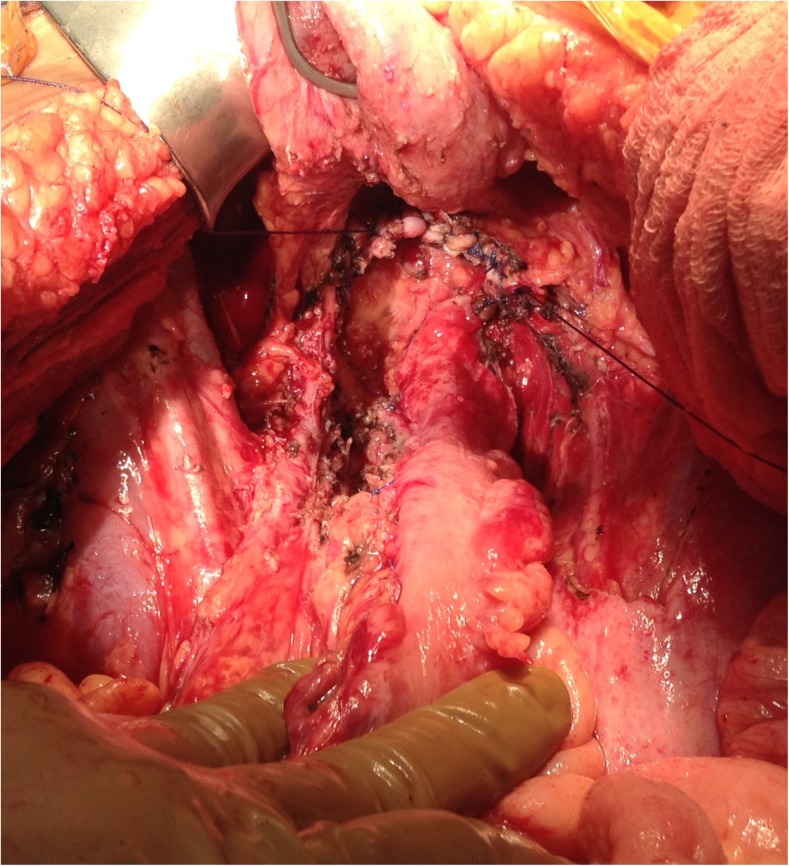
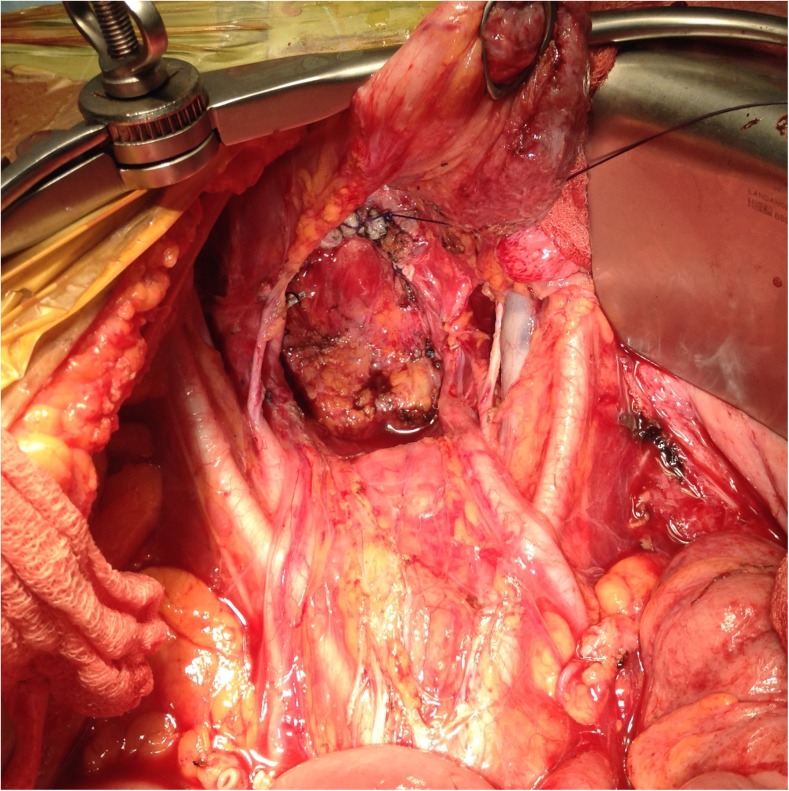
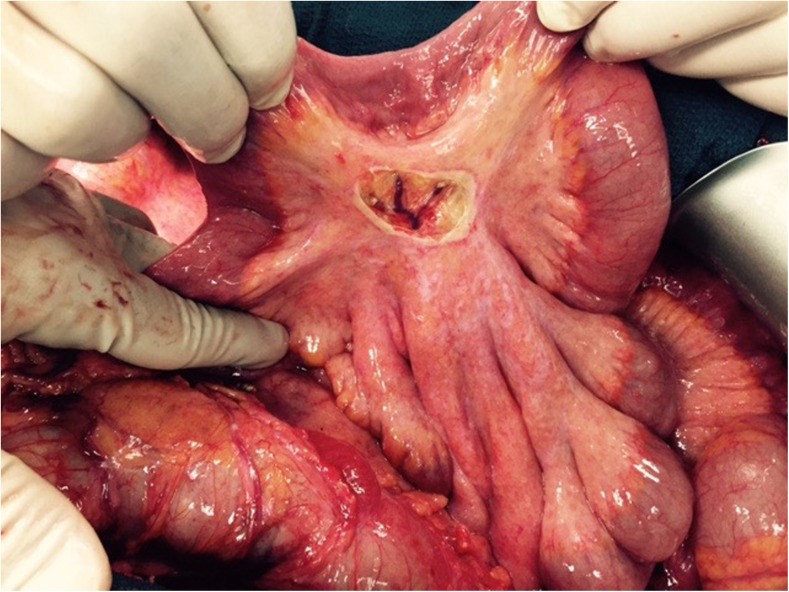
Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) has become widely accepted as an effective method of treating peritoneal metastases (PM) from various cancers. CRS performed with the goal of removing all the macroscopic disease and comprises of peritonectomy procedures and visceral resections. CRS is a technically challenging surgery that requires a considerable amount of skill and appropriate patient selection. This article is a review of the techniques and current recommendations for performing CRS.
Keywords: Cytoreductive surgery; Multi-organ resection; Pelvic peritonectomy; Peritonectomy; Subphrenic peritonectomy; Techniques of cytoreductive surgery.
Figures



References
-
- Sugarbaker PH. Management of peritoneal metastases - Basic concepts. J BUON. 2015;20(Suppl 1):S2–11. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources