

Insulin Is a Key Modulator of Fetoplacental Endothelium Metabolic Disturbances in Gestational Diabetes Mellitus
- PMID: 27065887
- PMCID: PMC4815008
- DOI: 10.3389/fphys.2016.00119
Insulin Is a Key Modulator of Fetoplacental Endothelium Metabolic Disturbances in Gestational Diabetes Mellitus
Abstract
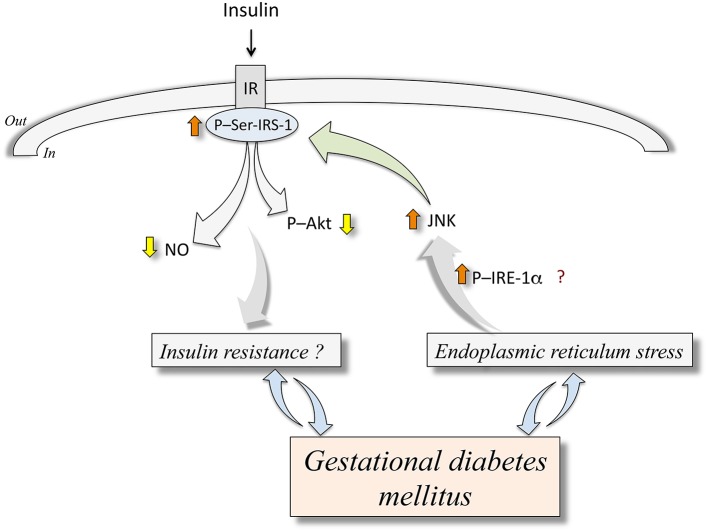
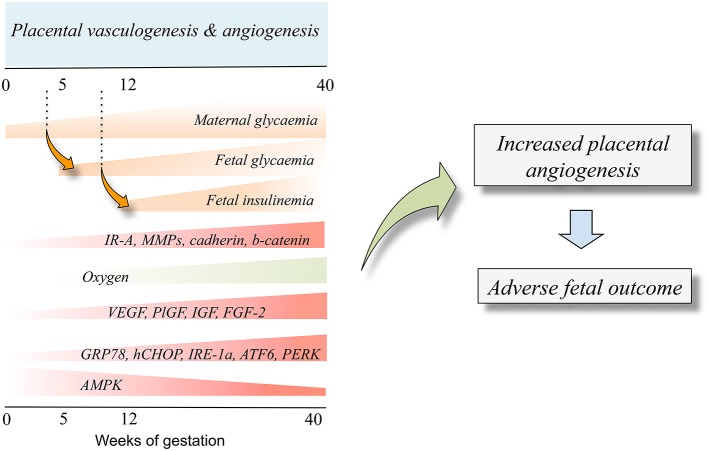
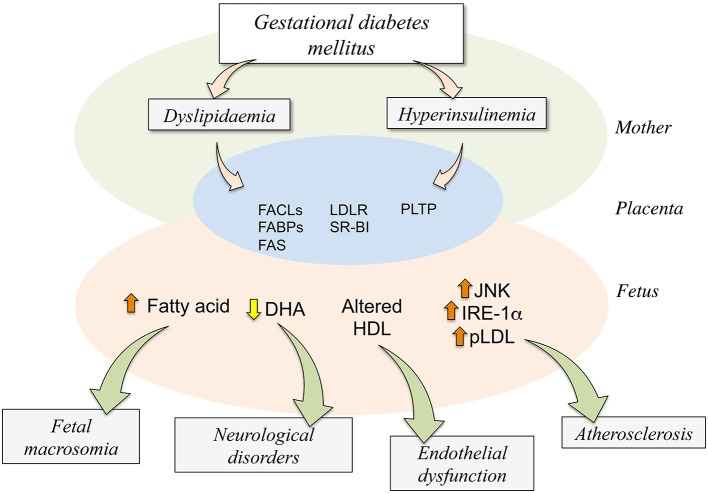
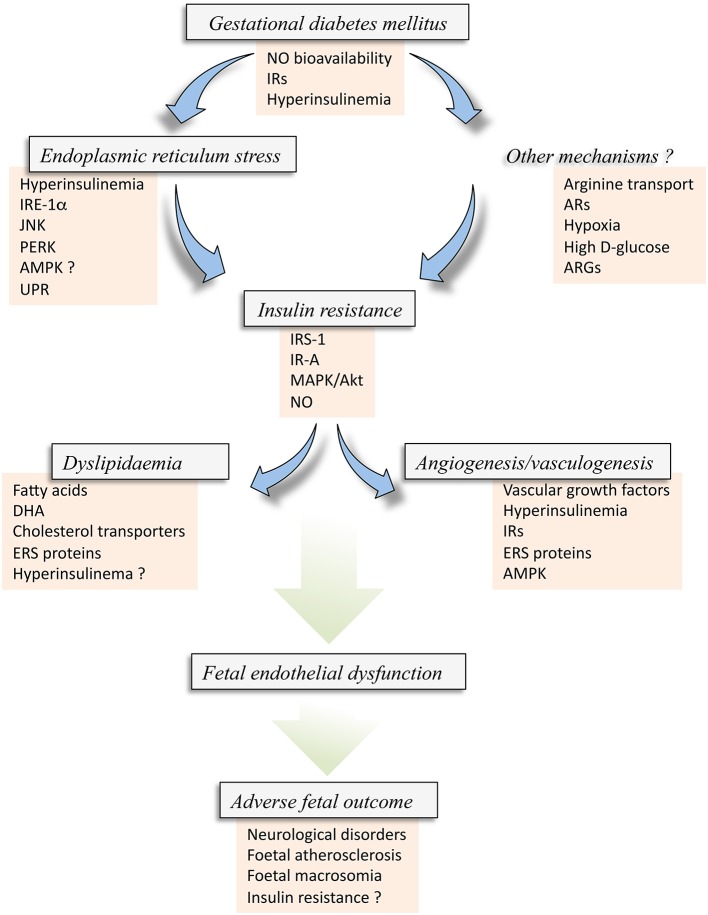
Gestational diabetes mellitus (GDM) is a disease of the mother that associates with altered fetoplacental vascular function. GDM-associated maternal hyperglycaemia result in fetal hyperglycaemia, a condition that leads to fetal hyperinsulinemia and altered L-arginine transport and synthesis of nitric oxide, i.e., endothelial dysfunction. These alterations in the fetoplacental endothelial function are present in women with GDM that were under diet or insulin therapy. Since these women and their newborn show normal glycaemia at term, other factors or conditions could be altered and/or not resolved by restoring normal level of circulating D-glucose. GDM associates with metabolic disturbances, such as abnormal handling of the locally released vasodilator adenosine, and biosynthesis and metabolism of cholesterol lipoproteins, or metabolic diseases resulting in endoplasmic reticulum stress and altered angiogenesis. Insulin acts as a potent modulator of all these phenomena under normal conditions as reported in primary cultures of cells obtained from the human placenta; however, GDM and the role of insulin regarding these alterations in this disease are poorly understood. This review focuses on the potential link between insulin and endoplasmic reticulum stress, hypercholesterolemia, and angiogenesis in GDM in the human fetoplacental vasculature. Based in reports in primary culture placental endothelium we propose that insulin is a factor restoring endothelial function in GDM by reversing ERS, hypercholesterolaemia and angiogenesis to a physiological state involving insulin activation of insulin receptor isoforms and adenosine receptors and metabolism in the human placenta from GDM pregnancies.
Keywords: angiogenesis; endoplasmic reticulum stress; endothelium; gestational diabetes; insulin; lipids; placenta.
Figures
Similar articles
-
Insulin therapy and fetoplacental vascular function in gestational diabetes mellitus.Exp Physiol. 2015 Mar;100(3):231-8. doi: 10.1113/expphysiol.2014.082743. Epub 2015 Feb 9. Exp Physiol. 2015. PMID: 25581778 Review.
-
Role of insulin, adenosine, and adipokine receptors in the foetoplacental vascular dysfunction in gestational diabetes mellitus.Biochim Biophys Acta Mol Basis Dis. 2020 Feb 1;1866(2):165370. doi: 10.1016/j.bbadis.2018.12.021. Epub 2019 Jan 17. Biochim Biophys Acta Mol Basis Dis. 2020. PMID: 30660686 Review.
-
Role of insulin and adenosine in the human placenta microvascular and macrovascular endothelial cell dysfunction in gestational diabetes mellitus.Microcirculation. 2014 Jan;21(1):26-37. doi: 10.1111/micc.12077. Microcirculation. 2014. PMID: 23875992 Review.
-
High total cholesterol and triglycerides levels increase arginases metabolism, impairing nitric oxide signaling and worsening fetoplacental endothelial dysfunction in gestational diabetes mellitus pregnancies.Biochim Biophys Acta Mol Basis Dis. 2021 Dec 1;1867(12):166216. doi: 10.1016/j.bbadis.2021.166216. Epub 2021 Jul 24. Biochim Biophys Acta Mol Basis Dis. 2021. PMID: 34314821
-
Functional link between adenosine and insulin: a hypothesis for fetoplacental vascular endothelial dysfunction in gestational diabetes.Curr Vasc Pharmacol. 2011 Nov;9(6):750-62. doi: 10.2174/157016111797484062. Curr Vasc Pharmacol. 2011. PMID: 22022830 Review.
Cited by
-
Adipose stem cells-derived small extracellular vesicles transport Thrombospondin 1 cargo to promote insulin resistance in gestational diabetes mellitus.Diabetol Metab Syndr. 2024 May 19;16(1):105. doi: 10.1186/s13098-024-01276-1. Diabetol Metab Syndr. 2024. PMID: 38764083 Free PMC article.
-
Identification and validation of the miRNA-mRNA regulatory network in fetoplacental arterial endothelial cells of gestational diabetes mellitus.Bioengineered. 2021 Dec;12(1):3503-3515. doi: 10.1080/21655979.2021.1950279. Bioengineered. 2021. PMID: 34233591 Free PMC article.
-
Identification and characterization of signature genes related to fetoplacental vascular endothelial cell programming in gestational diabetes mellitus using bioinformatics analysis.Front Genet. 2025 Jul 14;16:1600756. doi: 10.3389/fgene.2025.1600756. eCollection 2025. Front Genet. 2025. PMID: 40727584 Free PMC article.
-
The WWOX/HIF1A Axis Downregulation Alters Glucose Metabolism and Predispose to Metabolic Disorders.Int J Mol Sci. 2022 Mar 19;23(6):3326. doi: 10.3390/ijms23063326. Int J Mol Sci. 2022. PMID: 35328751 Free PMC article.
-
Low molecular weight heparin (nadroparin) improves placental permeability in rats with gestational diabetes mellitus via reduction of tight junction factors.Mol Med Rep. 2020 Feb;21(2):623-630. doi: 10.3892/mmr.2019.10868. Epub 2019 Dec 6. Mol Med Rep. 2020. PMID: 31974593 Free PMC article.
References
-
- Aguayo C., Flores C., Parodi J., Rojas R., Mann G. E., Pearson J. D., et al. (2001). Modulation of adenosine transport by insulin in human umbilical artery smooth muscle cells from normal or gestational diabetic pregnancies. J. Physiol. (Lond.) 534, 243–254. 10.1111/j.1469-7793.2001.00243.x - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources