Cholestasis beyond the Neonatal and Infancy Periods
- PMID: 27066444
- PMCID: PMC4821977
- DOI: 10.5223/pghn.2016.19.1.1
Cholestasis beyond the Neonatal and Infancy Periods
Abstract
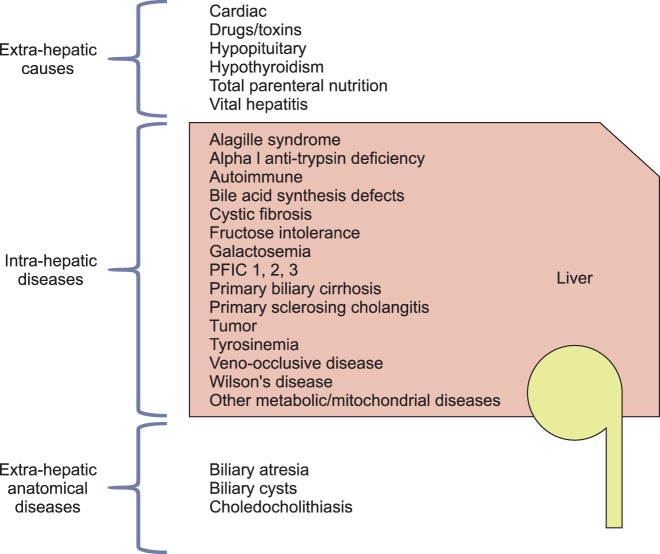
Cholestasis results from impairment in the excretion of bile, which may be due to mechanical obstruction of bile flow or impairment of excretion of bile components into the bile canaliculus. When present, cholestasis warrants prompt diagnosis and treatment. The differential diagnosis of cholestasis beyond the neonatal period is broad and includes congenital and acquired etiologies. It is imperative that the clinician differentiates between intrahepatic and extrahepatic origin of cholestasis. Treatment may be supportive or curative and depends on the etiology. Recent literature shows that optimal nutritional and medical support also plays an integral role in the management of pediatric patients with chronic cholestasis. This review will provide a broad overview of the pathophysiology, diagnostic approach, and management of cholestasis beyond the neonatal and infancy periods.
Keywords: Alagille syndrome; Biliary cysts; Cholelithiasis; Cholestasis; Conjugated hyperbilirubinemia; Hepatitis; Hepatolenticular degeneration; Jaundice; Pruritus.
Figures



References
-
- Suchy FJ, Sokol RJ, Balistreri WF. Liver disease in children. New York: Cambridge University Press; 2014.
-
- Kremer AE, Bolier R, van Dijk R, Oude Elferink RP, Beuers U. Advances in pathogenesis and management of pruritus in cholestasis. Dig Dis. 2014;32:637–645. - PubMed
-
- Chappell LC, Gurung V, Seed PT, Chambers J, Williamson C, Thornton JG PITCH Study Consortium. Ursodeoxycholic acid versus placebo, and early term delivery versus expectant management, in women with intrahepatic cholestasis of pregnancy: semifactorial randomised clinical trial. BMJ. 2012;344:e3799. - PMC - PubMed
-
- Kronsten V, Fitzpatrick E, Baker A. Management of cholestatic pruritus in paediatric patients with alagille syndrome: the King's College Hospital experience. J Pediatr Gastroenterol Nutr. 2013;57:149–154. - PubMed
-
- Moyer V, Freese DK, Whitington PF, Olson AD, Brewer F, Colletti RB, et al. North American Society for Pediatric Gastroenterology; Hepatology and Nutrition. Guideline for the evaluation of cholestatic jaundice in infants: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2004;39:115–128. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources