

Aortic valve replacement in elderly with small aortic root and low body surface area; the Perceval S valve and its impact in effective orifice area
- PMID: 27066903
- PMCID: PMC4827171
- DOI: 10.1186/s13019-016-0438-7
Aortic valve replacement in elderly with small aortic root and low body surface area; the Perceval S valve and its impact in effective orifice area
Abstract
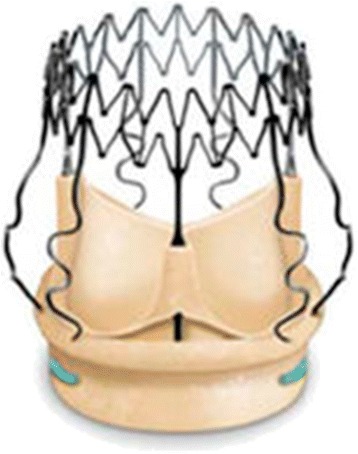
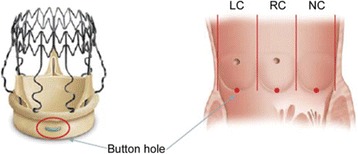
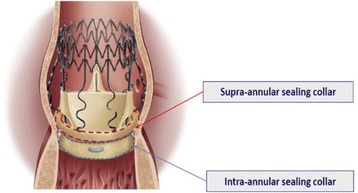
Background: The aim of this study is to see how the sutureless, stentless, Perceval S aortic valves behave when implanted in elderly patients with small aortic root and the comparison with a second group of patients with similar characteristics where a conventional stented bioprosthesis was implanted. This is a prospective randomized institutional study.
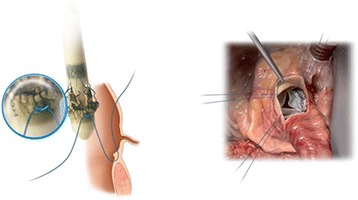
Methods: Our material is composed from 25 patients who underwent aortic valve replacement with sutureless self-anchoring Perceval S valve implantation (LivaNova), compared with 25 patients with conventional stented biological prosthesis implanted (soprano LivaNova group). The two groups of patients have similar demographic and medical characteristics with severe aortic stenosis. The study was conducted from January 2012 to June 2014. Preoperative, intraoperative and postoperative parameters were studied in order to investigate the utility of the Perceval S valves in this group of patients.
Results: The Perceval S valve implantation seems to be an interesting biological valve with good hemodynamic characteristics as compared with the typical biological prosthesis providing shorter ischemia time (40 ± 5.50 min vs 86 ± 15.86 min; p < 0.001), shorter extracorporeal circulation time (73.75 ± 8.12 min vs 120.36 ± 28.31 min p < 0.001), less operation time (149.38 ± 15.22 min vs 206.64 ± 42.85 min; p < 0.001) and better postoperative recovery. The postoperative gradients were 23.5 ± 19.20 mmHg vs 24.5 ± 19.90 mmHg respectively. The postoperative effective orifice area in these two groups were respectively 1.5 =/-0.19 cm(2) vs 1.1=/-0.5 cm(2) (p 0.002). Among the 25 patients of the Soprano stented valve, 3 (12 %) came back in 6 months with New York Heart Association (NYHA) 3. The PPM of these patients was the cause of readmission in the Hospital required diuresis and supplementary treatment.
Conclusions: Aortic valve replacement with Perceval aortic valves in geriatric patients with comorbidities and small aortic annulus seems to be an alternative, safe and "fast" intervention with excellent short and mid-term results which provides a better effective orifice area.
Keywords: Aortic valve; Aortic valve stenosis; Heart valve surgery; Perceval S; Self-expanding valve; Stentless aortic valve; Sutureless valve.
Figures


References
-
- Shrestha M, Foliiguet T, Meuris B, Dibie A, Bara C, Herregods MC, Meuris B, et al. Suturuless Perceval S aortic valve replacement: a multicenter, prospective pilot trial. J Heart Valve Dis. 2009;18:698–702. - PubMed
-
- David TE, Feindel CM, Bos J, Sun Z, Scully HE, Rakowski H. Aortic Valve replacement with a stentless porcine aortic valve. A six-year experience. J Cardiovasc Surg. 1994;108:1030–1036. - PubMed
-
- Apostolakis E, Baikoussis NG, Papakonstantinou NA, Goudevenos J. Patient-prosthesis mismatch and strategies to prevent it during aortic valve replacement. Hellenic J Cardiol. 2011;52(1):41–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
