

Regional variation exists in patient selection and treatment of abdominal aortic aneurysms
- PMID: 27066949
- PMCID: PMC5036976
- DOI: 10.1016/j.jvs.2016.02.036
Regional variation exists in patient selection and treatment of abdominal aortic aneurysms
Abstract
Objective: Significant regional variation in surgical rates has been identified following multiple surgical procedures. However, limited data have examined the regional variability in patient selection and treatment of abdominal aortic aneurysms (AAAs). This study aimed to evaluate regional variation in patient selection, perioperative management, and operative approach for the repair of AAAs.
Methods: All patients undergoing open repair or endovascular aneurysm repair (EVAR) of an AAA in the Vascular Quality Initiative from 2009 to 2014 were identified. All regional groups were deidentified, and those with fewer than 100 open repairs were combined into a single region.
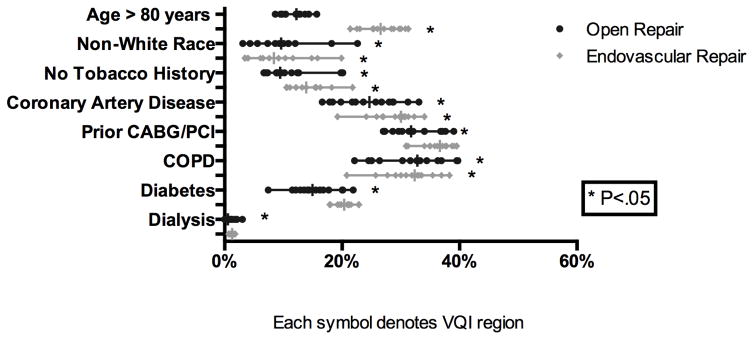
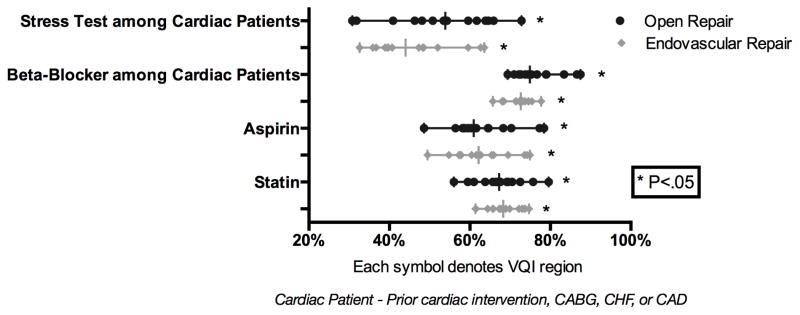
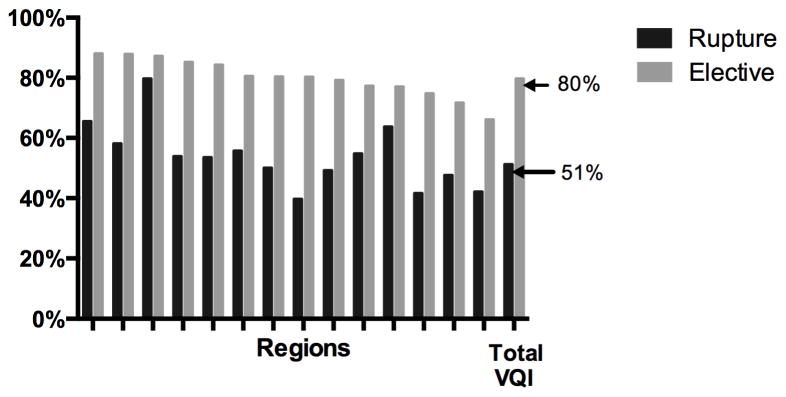
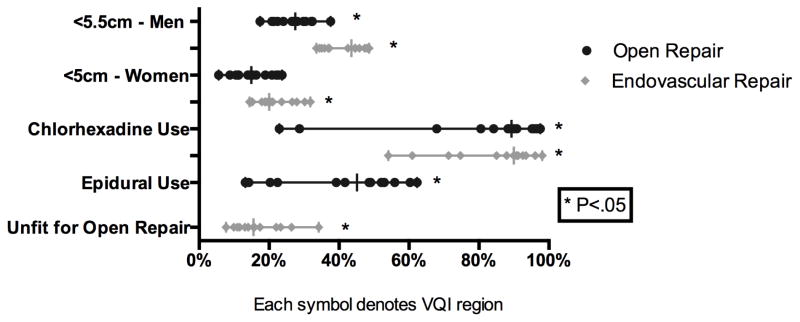
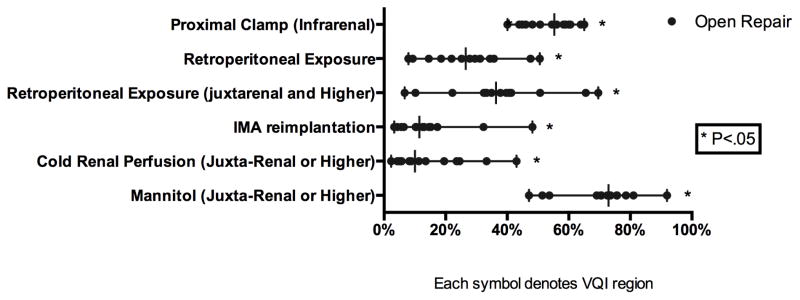
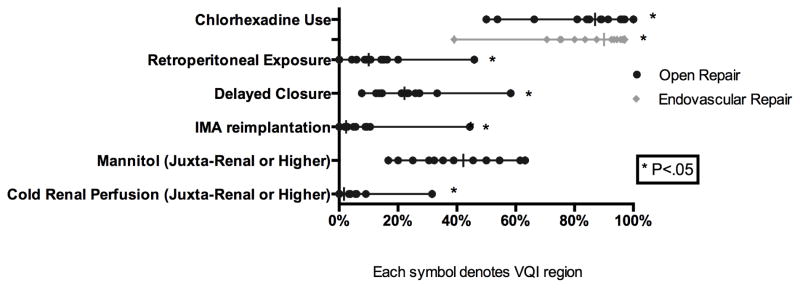
Results: We identified 17,269 elective repairs (EVAR, 13,759; open, 3510) and 1462 ruptured AAAs (EVAR, 749; open, 713). There was significant regional variation in the use of EVAR for elective repair (range, 66%-88%; P < .01) and ruptured AAA repair (40%-80%; P < .01). The median diameter for elective repair was similar among regions (EVAR, 5.4 cm; open, 5.7 cm). There was wide variation in the treatment of small aneurysms in male patients (<5.5 cm) for EVAR (34%-49%; P < .01) and open repair (17%-38%; P < .01) and variation in the treatment of small aneurysms in female patients (<5 cm) for EVAR (14%-32%; P < .01) but not significant for open repair (6%-24%). For elective cases, preoperative aspirin (EVAR, 50%-75% [P < .01]; open, 49%-78% [P < .01]) and statin use (EVAR, 61%-75% [P < .01]; open, 56%-80% [P < .01]) varied widely. Among elective cardiac patients, preoperative management varied significantly, including beta-blocker use (EVAR, 66%-78% [P < .01]; open, 69%-88% [P = .01]) and the frequency of stress tests (EVAR, 33%-64% [P < .01]; open, 31%-73% [P < .01]). Among open repairs for aneurysms extending at or beyond the juxtarenal segment, there was wide variation in the use of retroperitoneal exposures (7%-70%; P < .01) and adjunctive renal protective measures (cold renal perfusion, 2%-43% [P < .01]; mannitol, 47%-92% [P < .01]).
Conclusions: Significant regional variation exists in patient selection, perioperative management, and operative approach for the repair of AAA. Definitive evidence is lacking in many aspects of operative care, including the use of the retroperitoneal approach and renal protective strategies. However, this variation emphasizes the importance of research to determine best practice in the areas of greatest variation. Furthermore, where current clinical process measures exist and data are clear, such as the use of statin and antiplatelet agents, the high degree of variation should serve as an impetus for regional quality improvement projects.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Significant regional variation exists in morbidity and mortality after repair of abdominal aortic aneurysm.J Vasc Surg. 2017 May;65(5):1305-1312. doi: 10.1016/j.jvs.2016.08.110. Epub 2016 Nov 23. J Vasc Surg. 2017. PMID: 27887854 Free PMC article.
-
Outcomes for symptomatic abdominal aortic aneurysms in the American College of Surgeons National Surgical Quality Improvement Program.J Vasc Surg. 2016 Aug;64(2):297-305. doi: 10.1016/j.jvs.2016.02.055. Epub 2016 Apr 14. J Vasc Surg. 2016. PMID: 27146791 Free PMC article.
-
Patient selection and perioperative outcomes are similar between targeted and nontargeted hospitals (in the National Surgical Quality Improvement Program) for abdominal aortic aneurysm repair.J Vasc Surg. 2017 Feb;65(2):362-371. doi: 10.1016/j.jvs.2016.04.066. Epub 2016 Jul 25. J Vasc Surg. 2017. PMID: 27462004 Free PMC article.
-
Changes in abdominal aortic aneurysm epidemiology.J Cardiovasc Surg (Torino). 2017 Dec;58(6):848-853. doi: 10.23736/S0021-9509.17.10064-9. Epub 2017 Jun 20. J Cardiovasc Surg (Torino). 2017. PMID: 28633519 Review.
-
Randomized clinical trials of endovascular repair versus surveillance for treatment of small abdominal aortic aneurysms.J Endovasc Ther. 2009 Feb;16 Suppl 1:I94-105. doi: 10.1583/08-2600.1. J Endovasc Ther. 2009. PMID: 19317579 Review.
Cited by
-
2022 ACC/AHA guideline for the diagnosis and management of aortic disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines.J Thorac Cardiovasc Surg. 2023 Nov;166(5):e182-e331. doi: 10.1016/j.jtcvs.2023.04.023. Epub 2023 Jun 28. J Thorac Cardiovasc Surg. 2023. PMID: 37389507 Free PMC article.
-
2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines.J Am Coll Cardiol. 2022 Dec 13;80(24):e223-e393. doi: 10.1016/j.jacc.2022.08.004. Epub 2022 Nov 2. J Am Coll Cardiol. 2022. PMID: 36334952 Free PMC article.
-
Regional variation in patient selection and treatment for carotid artery disease in the Vascular Quality Initiative.J Vasc Surg. 2017 Jul;66(1):112-121. doi: 10.1016/j.jvs.2017.01.023. Epub 2017 Mar 27. J Vasc Surg. 2017. PMID: 28359719 Free PMC article.
-
Significant regional variation exists in morbidity and mortality after repair of abdominal aortic aneurysm.J Vasc Surg. 2017 May;65(5):1305-1312. doi: 10.1016/j.jvs.2016.08.110. Epub 2016 Nov 23. J Vasc Surg. 2017. PMID: 27887854 Free PMC article.
-
Epidemiology of endovascular and open repair for abdominal aortic aneurysms in the United States from 2004 to 2015 and implications for screening.J Vasc Surg. 2021 Aug;74(2):414-424. doi: 10.1016/j.jvs.2021.01.044. Epub 2021 Feb 14. J Vasc Surg. 2021. PMID: 33592293 Free PMC article.
References
-
- Hanstede MM, Burger MJ, Timmermans A, Burger MP. Regional and temporal variation in hysterectomy rates and surgical routes for benign diseases in the Netherlands. Acta Obstet Gynecol Scand. 2012;91(2):220–5. - PubMed
-
- Goodney PR, Dzebisashvili N, Goodman DC, Bronner KK. Variation in the Care of Surgical Conditions. The Dartmouth Institute for Health Policy and Clinical Practice; 2015. - PubMed
-
- McCulloch P, Nagendran M, Campbell WB, Price A, Jani A, Birkmeyer JD, et al. Strategies to reduce variation in the use of surgery. Lancet. 2013;382(9898):1130–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
