

The value of early and comprehensive diagnoses in a human fetus with hydrocephalus and progressive obliteration of the aqueduct of Sylvius: Case Report
- PMID: 27067115
- PMCID: PMC4828774
- DOI: 10.1186/s12883-016-0566-7
The value of early and comprehensive diagnoses in a human fetus with hydrocephalus and progressive obliteration of the aqueduct of Sylvius: Case Report
Abstract
Background: Mutant rodent models have highlighted the importance of the ventricular ependymal cells and the subcommissural organ (a brain gland secreting glycoproteins into the cerebrospinal fluid) in the development of fetal onset hydrocephalus. Evidence indicates that communicating and non-communicating hydrocephalus can be two sequential phases of a single pathological phenomenon triggered by ependymal disruption and/or abnormal function of the subcommissural organ. We have hypothesized that a similar phenomenon may occur in human cases with fetal onset hydrocephalus.
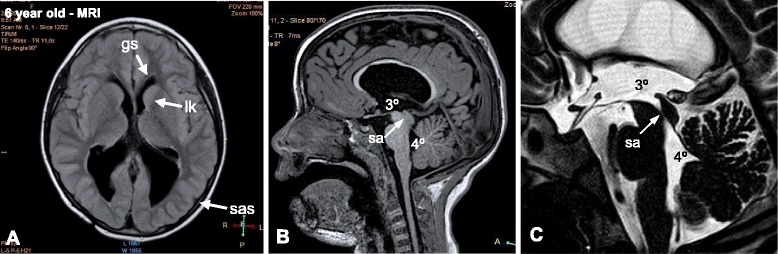
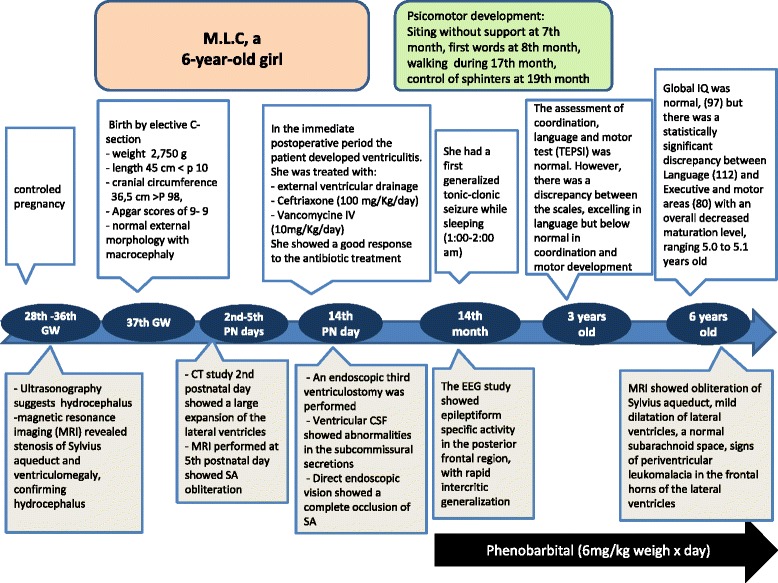
Case presentation: We report here on a case of human fetal communicating hydrocephalus with no central nervous system abnormalities other than stenosis of the aqueduct of Sylvius (SA) that became non-communicating hydrocephalus during the first postnatal week due to obliteration of the cerebral aqueduct. The case was followed closely by a team of basic and clinic investigators allowing an early diagnosis and prediction of the evolving pathophysiology. This information prompted neurosurgeons to perform a third ventriculostomy at postnatal day 14. The fetus was monitored by ultrasound, computerized axial tomography and magnetic resonance imaging (MRI). After birth, the follow up was by MRI, electroencephalography and neurological and neurocognitive assessments. Cerebrospinal fluid (CSF) collected at surgery showed abnormalities in the subcommissural organ proteins and the membrane proteins L1-neural cell adhesion molecule and aquaporin-4. The neurological and neurocognitive assessments at 3 and 6 years of age showed neurological impairments (epilepsy and cognitive deficits).
Conclusions: (1) In a hydrocephalic fetus, a stenosed SA can become obliterated at perinatal stages. (2) In the case reported, a close follow up of a communicating hydrocephalus detected in utero allowed a prompt postnatal surgery aiming to avoid as much brain damage as possible. (3) The clinical and pathological evolution of this patient supports the possibility that the progressive stenosis of the SA initiated during the embryonic period may have resulted from ependymal disruption of the cerebral aqueduct and dysfunction of the subcommissural organ. The analysis of subcommissural organ glycoproteins present in the CSF may be a valuable diagnostic tool for the pathogenesis of congenital hydrocephalus.
Keywords: Aqueduct of Sylvius; Case study; Cerebral aqueduct; Cerebrospinal fluid; Congenital hydrocephalus; Stenosis; Subcommissural organ.
Figures



References
-
- Del Bigio MR. Pathophysiologic consequences of hydrocephalus. Neurosurg Clin N Am. 2001;12:639–49. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
