

Changes in mortality inequalities over two decades: register based study of European countries
- PMID: 27067249
- PMCID: PMC4827355
- DOI: 10.1136/bmj.i1732
Changes in mortality inequalities over two decades: register based study of European countries
Abstract
Objective: To determine whether government efforts in reducing inequalities in health in European countries have actually made a difference to mortality inequalities by socioeconomic group.
Design: Register based study.
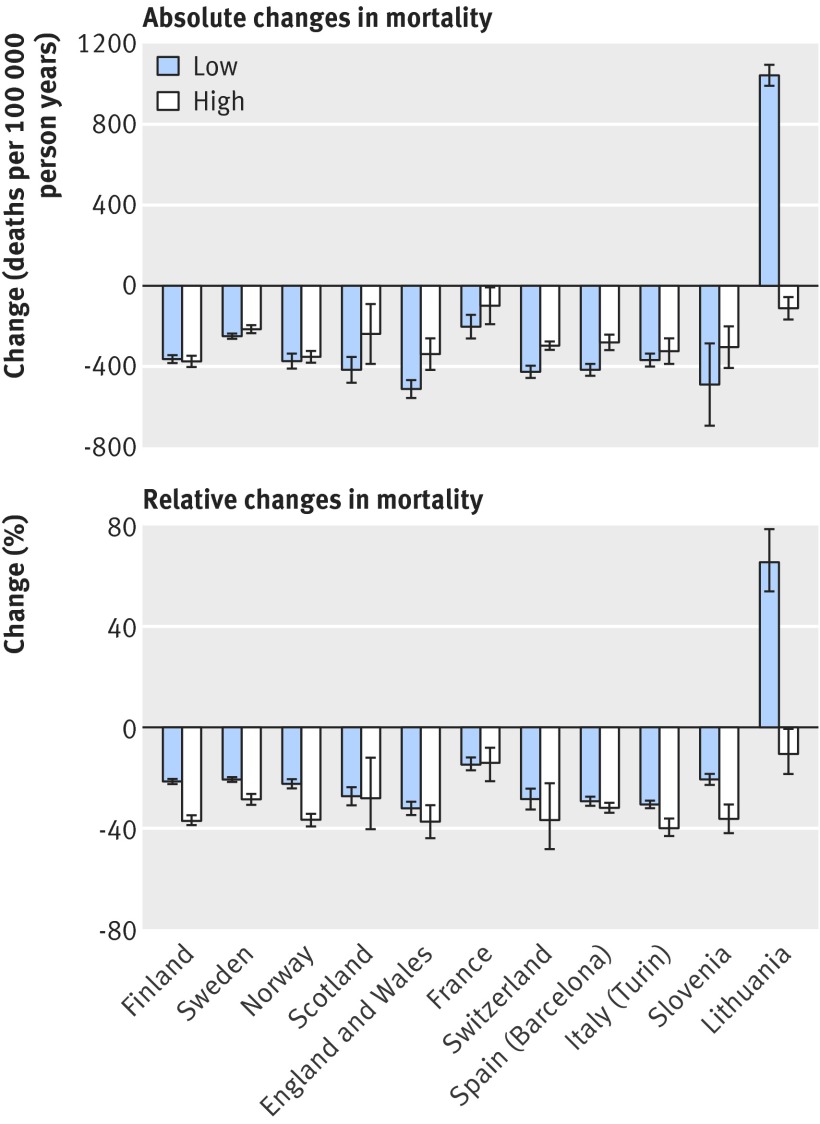
Data source: Mortality data by level of education and occupational class in the period 1990-2010, usually collected in a census linked longitudinal study design. We compared changes in mortality between the lowest and highest socioeconomic groups, and calculated their effect on absolute and relative inequalities in mortality (measured as rate differences and rate ratios, respectively).
Setting: All European countries for which data on socioeconomic inequalities in mortality were available for the approximate period between years 1990 and 2010. These included Finland, Norway, Sweden, Scotland, England and Wales (data applied to both together), France, Switzerland, Spain (Barcelona), Italy (Turin), Slovenia, and Lithuania.
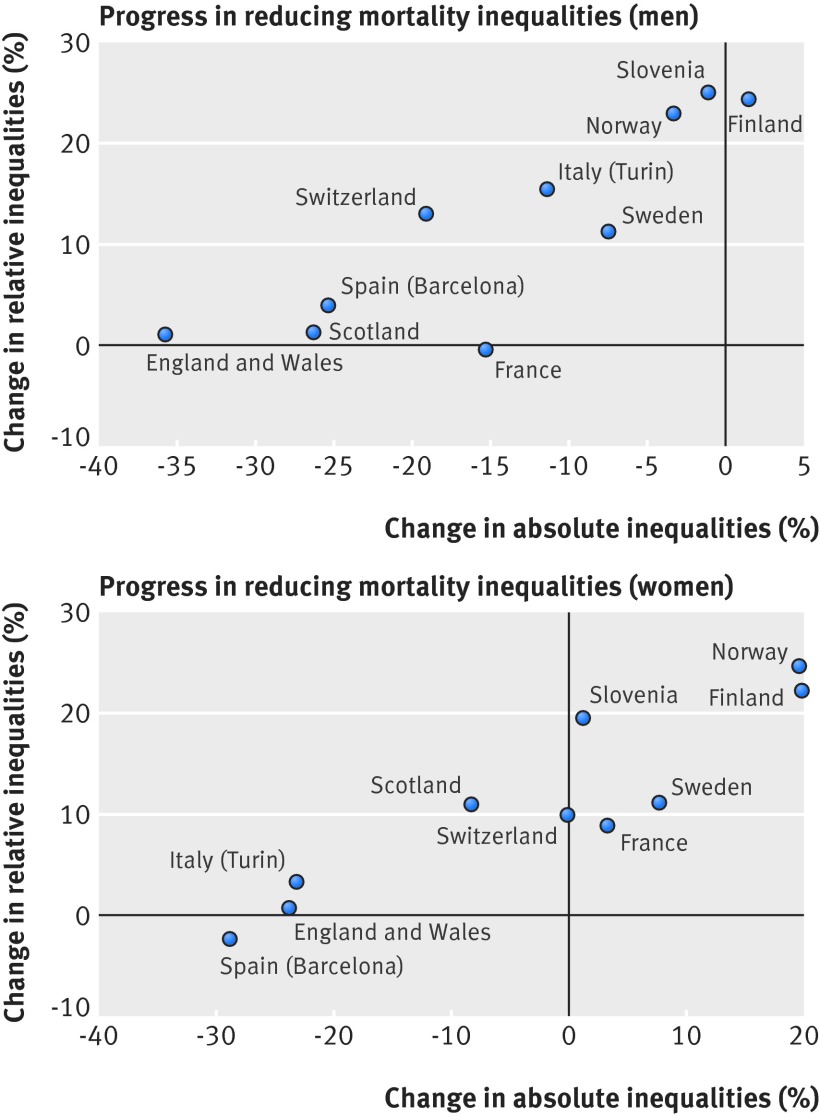
Results: Substantial mortality declines occurred in lower socioeconomic groups in most European countries covered by this study. Relative inequalities in mortality widened almost universally, because percentage declines were usually smaller in lower socioeconomic groups. However, as absolute declines were often smaller in higher socioeconomic groups, absolute inequalities narrowed by up to 35%, particularly among men. Narrowing was partly driven by ischaemic heart disease, smoking related causes, and causes amenable to medical intervention. Progress in reducing absolute inequalities was greatest in Spain (Barcelona), Scotland, England and Wales, and Italy (Turin), and absent in Finland and Norway. More detailed studies preferably using individual level data are necessary to identify the causes of these variations.
Conclusions: Over the past two decades, trends in inequalities in mortality have been more favourable in most European countries than is commonly assumed. Absolute inequalities have decreased in several countries, probably more as a side effect of population wide behavioural changes and improvements in prevention and treatment, than as an effect of policies explicitly aimed at reducing health inequalities.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures


References
-
- Commission on Social Determinants of Health. Closing the gap in a generation. Health equity through the social determinants of health. World Health Organization, 2008. - PubMed
-
- World Health Organization. Health21: the health for all policy framework for the WHO European Region. WHO Regional Office for Europe, 1999.
-
- Bauld L, Day P, Judge K. Off target: a critical review of setting goals for reducing health inequalities in the United Kingdom. Int J Health Serv 2008;38:439-54. 10.2190/HS.38.3.d pmid:18724576. - DOI - PubMed
-
- Jemal A, Ward E, Anderson RN, Murray T, Thun MJ. Widening of socioeconomic inequalities in US death rates, 1993-2001. PLoS One 2008;3:e2181 10.1371/journal.pone.0002181 pmid:18478119. - DOI - PMC - PubMed
-
- Tarkiainen L, Martikainen P, Laaksonen M, Valkonen T. Trends in life expectancy by income from 1988 to 2007: decomposition by age and cause of death. J Epidemiol Community Health 2012;66:573-8. 10.1136/jech.2010.123182 pmid:21378391. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous