

Electrocardiographic Left Ventricular Hypertrophy as a Predictor of Cardiovascular Disease Independent of Left Ventricular Anatomy in Subjects Aged ≥65 Years
- PMID: 27067620
- PMCID: PMC4867240
- DOI: 10.1016/j.amjcard.2016.03.020
Electrocardiographic Left Ventricular Hypertrophy as a Predictor of Cardiovascular Disease Independent of Left Ventricular Anatomy in Subjects Aged ≥65 Years
Abstract
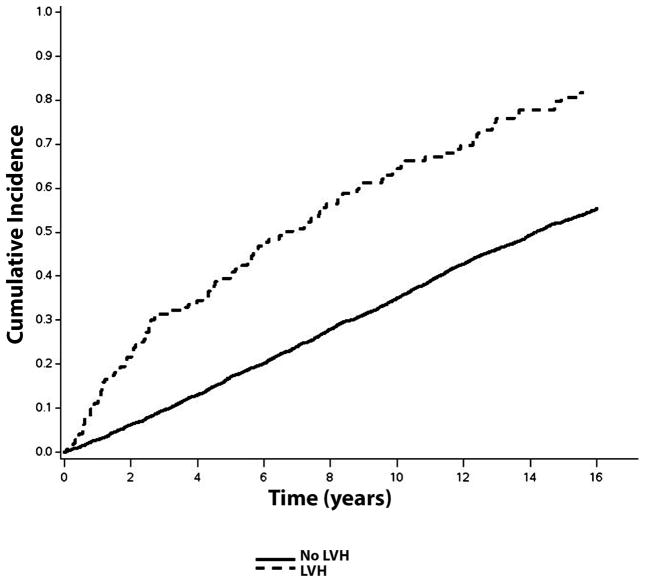
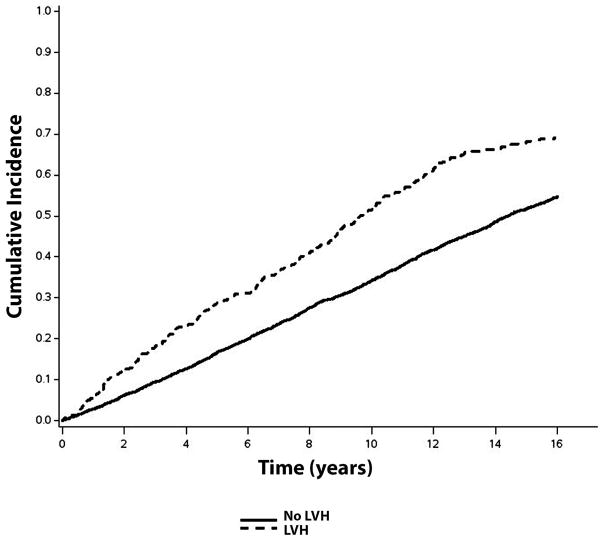
Left ventricular hypertrophy (LVH) diagnosed by electrocardiography (ECG-LVH) and echocardiography (echo-LVH) are independently associated with an increased risk of cardiovascular disease (CVD) events. However, it is unknown if ECG-LVH retains its predictive properties independent of LV anatomy. We compared the risk of CVD associated with ECG-LVH and echo-LVH in 4,076 participants (41% men, 86% white) from the Cardiovascular Health Study, who were free of baseline CVD. ECG-LVH was defined with Minnesota ECG Classification criteria from baseline ECG data. Echo-LVH was defined by gender-specific LV mass values normalized to body surface area (male: >102 g/m(2); female: >88 g/m(2)). ECG-LVH was detected in 144 participants (3.5%) and echo-LVH in 430 participants (11%). Over a median follow-up of 10.6 years, 2,274 CVD events occurred. In a multivariate Cox regression analysis adjusted for common CVD risk factors, ECG-LVH (hazard ratio [HR] 1.84, 95% CI 1.51 to 2.24) and echo-LVH (HR 1.35, 95% CI 1.19 to 1.54) were associated with an increased risk for CVD events. The association between ECG-LVH and CVD events was not substantively altered with further adjustment for echo-LVH (HR 1.76, 95% CI 1.45 to 2.15). In conclusion, the association of ECG-LVH with CVD events is not dependent on echo-LVH. This finding provides support to the concept that ECG-LVH is an electrophysiological marker with predictive properties independent of LV anatomy.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Bikkina M, Levy D, Evans JC, Larson MG, Benjamin EJ, Wolf PA, Castelli WP. Left ventricular mass and risk of stroke in an elderly cohort. The Framingham Heart Study. JAMA. 1994;272:33–36. - PubMed
-
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Left Ventricular Mass and Incidence of Coronary Heart Disease in an Elderly Cohort The Framingham Heart Study. Ann Intern Med. 1989;110:101–107. - PubMed
-
- Levy D, Salomon M, D’Agostino RB, Belanger AJ, Kannel WB. Prognostic implications of baseline electrocardiographic features and their serial changes in subjects with left ventricular hypertrophy. Circulation. 1994;90:1786–1793. - PubMed
-
- Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: a risk profile from the Framingham Study. Stroke. 1991;22:312–318. - PubMed
-
- Manolio TA, Kronmal RA, Burke GL, O’Leary DH, Price TR Group for the CCR. Short-term Predictors of Incident Stroke in Older Adults The Cardiovascular Health Study. Stroke. 1996;27:1479–1486. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
