

Incidence and In-Hospital Mortality of Acute Kidney Injury (AKI) and Dialysis-Requiring AKI (AKI-D) After Cardiac Catheterization in the National Inpatient Sample
- PMID: 27068629
- PMCID: PMC4943252
- DOI: 10.1161/JAHA.115.002739
Incidence and In-Hospital Mortality of Acute Kidney Injury (AKI) and Dialysis-Requiring AKI (AKI-D) After Cardiac Catheterization in the National Inpatient Sample
Abstract
Background: Acute kidney injury (AKI) and dialysis-requiring AKI (AKI-D) are common, serious complications of cardiac procedures.
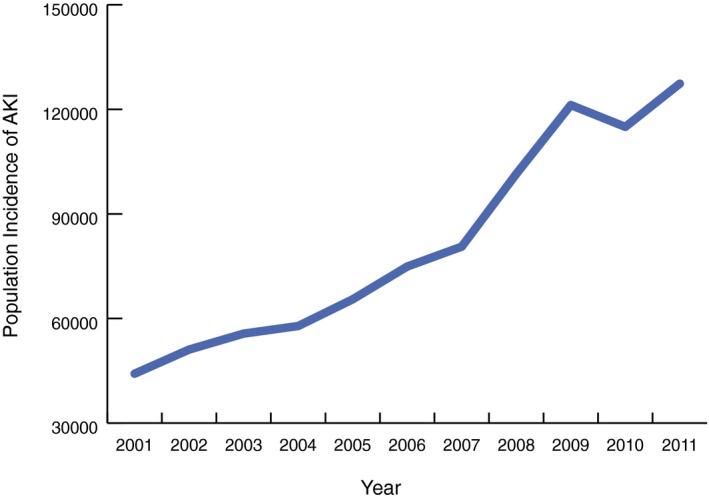
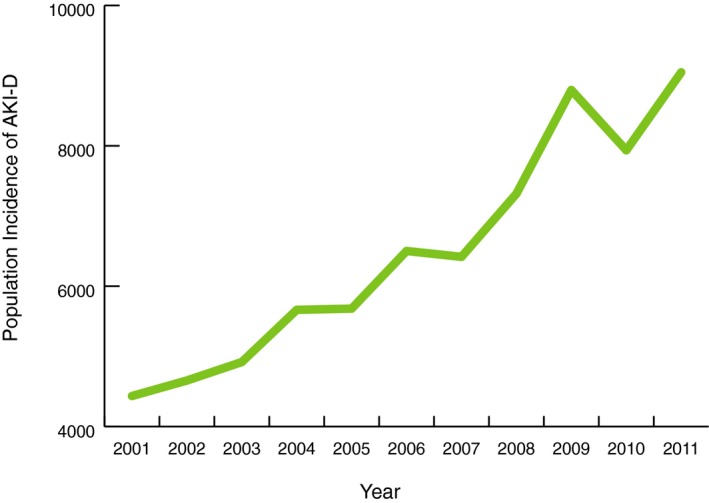
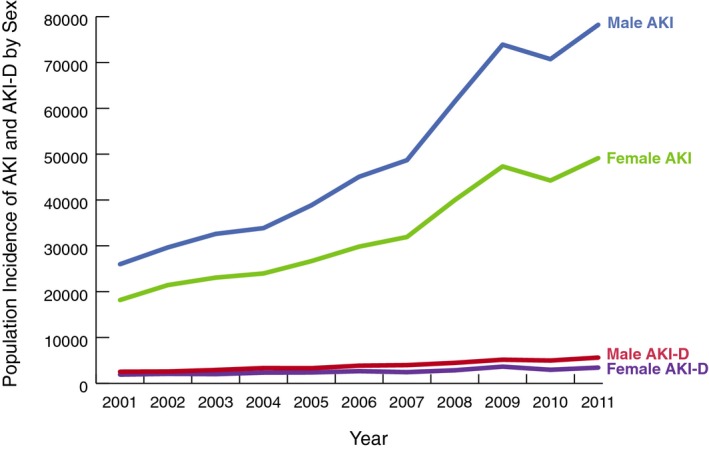
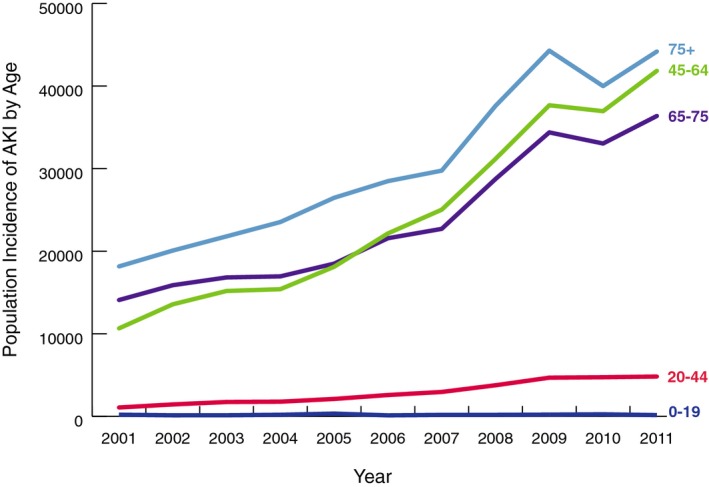
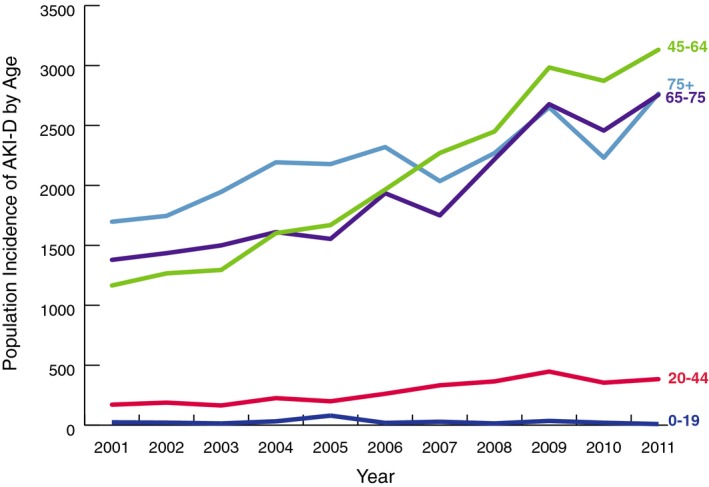
Methods and results: We evaluated 3 633 762 (17 765 214 weighted population) cardiac catheterization or percutaneous coronary intervention (PCI) hospital discharges from the nationally representative National Inpatient Sample to determine annual population incidence rates for AKI and AKI-D in the United States from 2001 to 2011. Odds ratios for both conditions and associated in-hospital mortality were calculated for each year in the study period using multiple logistic regression. The number of cardiac catheterization or PCI cases resulting in AKI rose almost 3-fold from 2001 to 2011. The adjusted odds of AKI and AKI-D per year among cardiac catheterization and PCI patients were 1.11 (95% CI: 1.10-1.12) and 1.01 (95% CI: 0.99-1.02), respectively. Most importantly, in-hospital mortality significantly decreased from 2001 to 2011 for AKI (19.6-9.2%) and AKI-D (28.3-19.9%), whereas odds of associated in-hospital mortality were 0.50 (95% CI: 0.45-0.56) and 0.70 (95% CI: 0.55-0.93) in 2011 versus 2001, respectively. The population-attributable risk of mortality for AKI and AKI-D was 25.8% and 3.8% in 2001 and 41.1% and 6.5% in 2011, respectively. Males and females had similar patterns of AKI increase, although males outpaced females.
Conclusions: The Incidence of AKI among cardiac catheterization and PCI patients has increased sharply in the United States, and this should be addressed by implementing prevention strategies. However, mortality has significantly declined, suggesting that efforts to manage AKI and AKI-D after cardiac catheterization and PCI have reduced mortality.
Keywords: acute kidney injury; acute renal failure; glomerular filtration rate; renal failure.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics–2013 update: a report from the American Heart Association. Circulation. 2013;127:e6–e245. - PMC - PubMed
-
- Hassan A, Newman A, Ko DT, Rinfret S, Hirsch G, Ghali WA, Tu JV. Increasing rates of angioplasty versus bypass surgery in Canada, 1994–2005. Am Heart J. 2010;160:958–965. - PubMed
-
- Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, Stahle E, Feldman TE, van den Brand M, Bass EJ, Van Dyck N, Leadley K, Dawkins KD, Mohr FW. Percutaneous coronary intervention versus coronary‐artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–972. - PubMed
-
- Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, Yang M, Cohen DJ, Rosenberg Y, Solomon SD, Desai AS, Gersh BJ, Magnuson EA, Lansky A, Boineau R, Weinberger J, Ramanathan K, Sousa JE, Rankin J, Bhargava B, Buse J, Hueb W, Smith CR, Muratov V, Bansilal S, King S III, Bertrand M, Fuster V. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367:2375–2384. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
