

Ethnicity, Socioeconomic Status, and Health Disparities in a Mixed Rural-Urban US Community-Olmsted County, Minnesota
- PMID: 27068669
- PMCID: PMC4871690
- DOI: 10.1016/j.mayocp.2016.02.011
Ethnicity, Socioeconomic Status, and Health Disparities in a Mixed Rural-Urban US Community-Olmsted County, Minnesota
Abstract
Objective: To characterize health disparities in common chronic diseases among adults by socioeconomic status (SES) and ethnicity in a mixed rural-urban community of the United States.
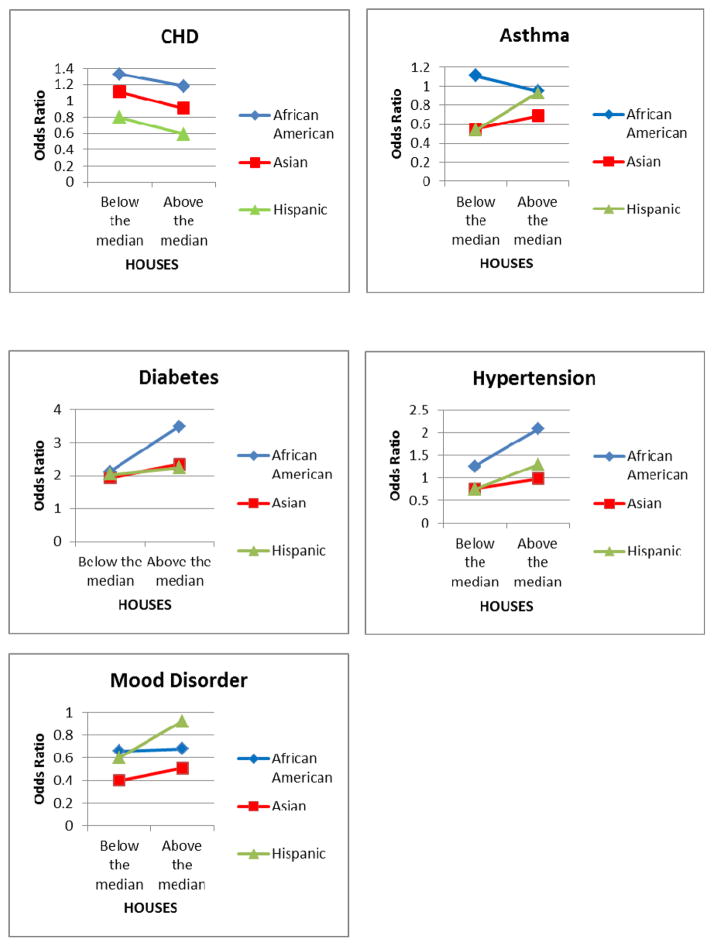
Patients and methods: We conducted a cross-sectional study to assess the association of the prevalence of the 5 most burdensome chronic diseases in adults with SES and ethnicity and their interaction. The Rochester Epidemiology Project medical records linkage system was used to identify the prevalence of coronary heart disease, asthma, diabetes, hypertension, and mood disorder using International Classification of Diseases, Ninth Revision codes recorded from January 1, 2005, through December 31, 2009, among all adult residents of Olmsted County, Minnesota, on April 1, 2009. For SES measurements, an individual HOUsing-based index of SocioEconomic Status (HOUSES) derived from real property data was used. Logistic regression models were used to examine the association of the prevalence of chronic diseases with ethnicity and HOUSES score and their interaction.
Results: We identified 88,010 eligible adults with HOUSES scores available, of whom 48,086 (54.6%) were female and 80,699 (91.7%) were non-Hispanic white; the median (interquartile range) age was 45 years (30-58 years). Overall and in the subgroup of non-Hispanic whites, SES measured by HOUSES was inversely associated with the prevalence of all 5 chronic diseases independent of age, sex, and ethnicity (P<.001). While an association of ethnicity with disease prevalence was observed for all the chronic diseases, SES modified the effect of ethnicity for clinically less overt conditions (interaction P<.05 for each condition [diabetes, hypertension, and mood disorder]) but not for coronary heart disease, a clinically more overt condition.
Conclusion: In a mixed rural-urban setting with a predominantly non-Hispanic white population, health disparities in chronic diseases still exist across SES. The extent to which SES modifies the effect of ethnicity on the risk of chronic diseases may depend on the nature of the disease.
Copyright © 2016 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Socioeconomic Status, Race/Ethnicity, and Health Disparities in Children and Adolescents in a Mixed Rural-Urban Community-Olmsted County, Minnesota.Mayo Clin Proc. 2019 Jan;94(1):44-53. doi: 10.1016/j.mayocp.2018.06.030. Mayo Clin Proc. 2019. PMID: 30611453 Free PMC article.
-
Disparities in Breast Cancer Survival by Socioeconomic Status Despite Medicare and Medicaid Insurance.Milbank Q. 2018 Dec;96(4):706-754. doi: 10.1111/1468-0009.12355. Milbank Q. 2018. PMID: 30537364 Free PMC article.
-
Glioma incidence and survival variations by county-level socioeconomic measures.Cancer. 2019 Oct 1;125(19):3390-3400. doi: 10.1002/cncr.32328. Epub 2019 Jun 17. Cancer. 2019. PMID: 31206646 Free PMC article.
-
The Role of Socioeconomic Status in Latino Health Disparities Among Youth with Type 1 Diabetes: a Systematic Review.Curr Diab Rep. 2020 Sep 25;20(11):56. doi: 10.1007/s11892-020-01346-4. Curr Diab Rep. 2020. PMID: 32974793
-
Disparities in Kidney Stone Disease: A Scoping Review.J Urol. 2021 Sep;206(3):517-525. doi: 10.1097/JU.0000000000001846. Epub 2021 Apr 27. J Urol. 2021. PMID: 33904797 Free PMC article.
Cited by
-
The relationship of 25-hydroxyvitamin D concentrations and individual-level socioeconomic status.J Steroid Biochem Mol Biol. 2020 Mar;197:105545. doi: 10.1016/j.jsbmb.2019.105545. Epub 2019 Nov 18. J Steroid Biochem Mol Biol. 2020. PMID: 31751783 Free PMC article.
-
Incidence of Respiratory Syncytial Virus in Community-Dwelling Adults Aged 18-64 Years Over 2 Seasons, 2022-2024, in a North American Community.Open Forum Infect Dis. 2024 Oct 11;11(10):ofae597. doi: 10.1093/ofid/ofae597. eCollection 2024 Oct. Open Forum Infect Dis. 2024. PMID: 39474445 Free PMC article.
-
The Relationship of Sleep Duration with Ethnicity and Chronic Disease in a Canadian General Population Cohort.Nat Sci Sleep. 2020 Apr 15;12:239-251. doi: 10.2147/NSS.S226834. eCollection 2020. Nat Sci Sleep. 2020. PMID: 32346318 Free PMC article.
-
Asthma and risk of glioma: a population-based case-control study.BMJ Open. 2019 Jun 17;9(6):e025746. doi: 10.1136/bmjopen-2018-025746. BMJ Open. 2019. PMID: 31213444 Free PMC article.
-
Epidemiology and outcomes of gastroparesis, as documented in general practice records, in the United Kingdom.Gut. 2021 Apr;70(4):644-653. doi: 10.1136/gutjnl-2020-321277. Epub 2020 Jun 3. Gut. 2021. PMID: 32493829 Free PMC article.
References
-
- [Accessed January 23th, 2015];Healthy People 2020. https://www.healthypeople.gov/
-
- Healthy People 2020 Leading Health Indicators: Progress Update. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion; 2014.
-
- Banks J, Marmot M, Oldfield Z, Smith JP. Disease and disadvantage in the United States and in England. Jama. 2006 May 3;295(17):2037–2045. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
