

Outcome of a cohort of severe cerebral venous thrombosis in intensive care
- PMID: 27068929
- PMCID: PMC4828343
- DOI: 10.1186/s13613-016-0135-7
Outcome of a cohort of severe cerebral venous thrombosis in intensive care
Erratum in
-
Erratum to: Outcome of a cohort of severe cerebral venous thrombosis in intensive care.Ann Intensive Care. 2016 Dec;6(1):108. doi: 10.1186/s13613-016-0209-6. Epub 2016 Nov 2. Ann Intensive Care. 2016. PMID: 27807820 Free PMC article. No abstract available.
Abstract
Background: Severity of cerebral venous thrombosis (CVT) may require the transfer to intensive care unit (ICU). This report described the context for CVT transfer to ICU, the strategy of care and the outcome after 1 year.
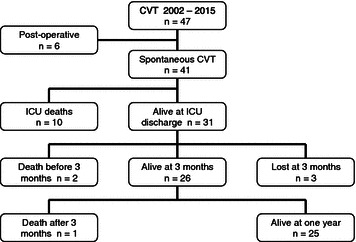
Methods: Monocentric cohort of 41 consecutive CVT admitted in a French ICU tertiary hospital (National Referent Center for CVT). Data collected are as follows: demographic data, clinical course, incidence of craniectomy and/or endovascular procedures and outcome in ICU, after 3 and 12 months.
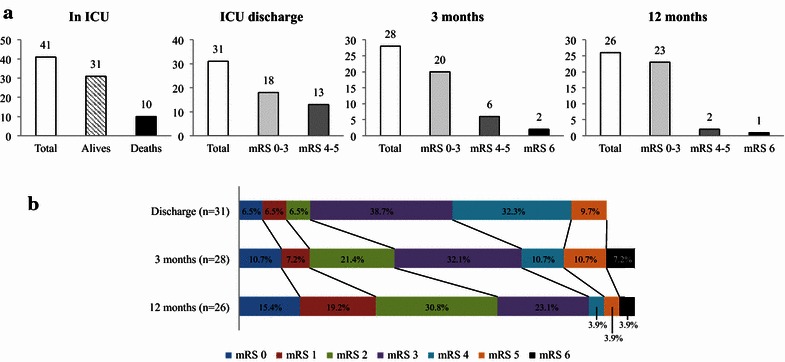
Results: 47 years old (IQ 26-53), with 73.2 % were female, having a SAPS II 41 (32-45), GCS 7 (5-8), and at least one episode of mydriasis in 48.8 %. Thrombosis location was 80.5 % in lateral sinus and 53.7 % in superior sagittal sinus; intracranial hematoma was present in 78.0 %, signs of intracranial hypertension in 60.9 %, cerebral edema in 58.5 % and venous ischemia in 43.9 %. All patients received heparin therapy, and 9 cases had endovascular treatment (21.9 %); osmotherapy (53.7 %) and decompressive craniectomy (16 cases, 39 %) necessary to control intracranial hypertension. Ten patients/41 (24.4 %) died in ICU and 18/31 (58.1 %) were discharged from ICU with outcome 0-3 of mRS. After 12 months, 92 % of survivors (23/25) had a mRS between 0 and 3. The proportion of death was 31.7 % at 1 year.
Conclusions: The large proportion of acceptable outcome in survivors, which continue to functionally improve after 1 year, motivates the hospitalization in ICU for severe CVT. For similar CVT severity, craniectomy did not improve outcome in comparison with the absence of craniectomy.
Keywords: Decompressive craniectomy; Endovascular therapies; Intracranial hematoma; Intracranial hypertension; Multimodal monitoring; Neuro-resuscitation; Severe cerebral venous thrombosis.
Figures
Similar articles
-
Decompressive craniectomy in severe cerebral venous and dural sinus thrombosis.Acta Neurochir Suppl. 2005;94:177-83. doi: 10.1007/3-211-27911-3_28. Acta Neurochir Suppl. 2005. PMID: 16060260 Clinical Trial.
-
Decompressive craniectomy in hemorrhagic cerebral venous thrombosis: clinicoradiological features and risk factors.J Neurosurg. 2017 Oct;127(4):709-715. doi: 10.3171/2016.8.JNS161112. Epub 2016 Oct 21. J Neurosurg. 2017. PMID: 27767398
-
Malignant Cerebral Venous Infarction: Decompressive Craniectomy versus Medical Treatment.World Neurosurg. 2019 Aug;128:e918-e922. doi: 10.1016/j.wneu.2019.05.028. Epub 2019 May 13. World Neurosurg. 2019. PMID: 31096029
-
Surgical Thrombectomy Combined with Bilateral Decompressive Craniectomy in a Life-Threatening Case of Coma from Cerebral Venous Sinus Thrombosis: Case Report and Literature Review.World Neurosurg. 2018 Dec;120:485-489. doi: 10.1016/j.wneu.2018.09.083. Epub 2018 Sep 22. World Neurosurg. 2018. PMID: 30253994 Review.
-
Timing of Anticoagulation in Patients with Cerebral Venous Thrombosis Requiring Decompressive Surgery: Systematic Review of the Literature and Case Series.World Neurosurg. 2020 May;137:408-414. doi: 10.1016/j.wneu.2020.02.084. Epub 2020 Feb 24. World Neurosurg. 2020. PMID: 32105874
Cited by
-
Balloon-Assisted Thrombectomy and Intrasinus Urokinase Thrombolysis for Severe Cerebral Venous Sinus Thrombosis.Front Neurol. 2021 Nov 18;12:735540. doi: 10.3389/fneur.2021.735540. eCollection 2021. Front Neurol. 2021. PMID: 34867719 Free PMC article.
-
Erratum to: Outcome of a cohort of severe cerebral venous thrombosis in intensive care.Ann Intensive Care. 2016 Dec;6(1):108. doi: 10.1186/s13613-016-0209-6. Epub 2016 Nov 2. Ann Intensive Care. 2016. PMID: 27807820 Free PMC article. No abstract available.
-
Update in Neurocritical Care: a summary of the 2018 Paris international conference of the French Society of Intensive Care.Ann Intensive Care. 2019 Apr 16;9(1):47. doi: 10.1186/s13613-019-0523-x. Ann Intensive Care. 2019. PMID: 30993550 Free PMC article. Review.
-
Surgical management of cerebral venous sinus thrombosis: Case series and literature review.Surg Neurol Int. 2021 Mar 30;12:133. doi: 10.25259/SNI_804_2020. eCollection 2021. Surg Neurol Int. 2021. PMID: 33880238 Free PMC article.
-
Role, Effectiveness, and Outcome of Decompressive Craniectomy for Cerebral Venous and Dural Sinus Thrombosis (CVST): Is Surgery Really an Option?Cureus. 2020 Dec 17;12(12):e12135. doi: 10.7759/cureus.12135. Cureus. 2020. PMID: 33489547 Free PMC article. Review.
References
-
- Einhäupl K, Stam J, Bousser M-G, De Bruijn SFTM, Ferro JM, Martinelli I, Masuhr F. EFNS guideline on the treatment of cerebral venous and sinus thrombosis in adult patients. Eur J Neurol Off J Eur Fed Neurol Soc. 2010;17:1229–1235. - PubMed
-
- Ferro JM, Bacelar-Nicolau H, Rodrigues T, Bacelar-Nicolau L, Canhão P, Crassard I, Bousser M-G, Dutra AP, Massaro A, Mackowiack-Cordiolani M-A, Leys D, Fontes J, Stam J, Barinagarrementeria F. Risk score to predict the outcome of patients with cerebral vein and dural sinus thrombosis. Cerebrovasc Dis Basel Switz. 2009;28:39–44. doi: 10.1159/000215942. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
