

Primary prevention of beta-cell autoimmunity and type 1 diabetes - The Global Platform for the Prevention of Autoimmune Diabetes (GPPAD) perspectives
- PMID: 27069865
- PMCID: PMC4811998
- DOI: 10.1016/j.molmet.2016.02.003
Primary prevention of beta-cell autoimmunity and type 1 diabetes - The Global Platform for the Prevention of Autoimmune Diabetes (GPPAD) perspectives
Abstract
Objective: Type 1 diabetes can be identified by the presence of beta-cell autoantibodies that often arise in the first few years of life. The purpose of this perspective is to present the case for primary prevention of beta-cell autoimmunity and to provide a study design for its implementation in Europe.
Methods: We examined and summarized recruitment strategies, enrollment rates, and outcomes in published TRIGR, FINDIA and BABYDIET primary prevention trials, and the TEDDY intensive observational study. A proposal for a recruitment and implementation strategy to perform a phase II/III primary prevention randomized controlled trial in infants with genetic risk for developing beta-cell autoimmunity is outlined.
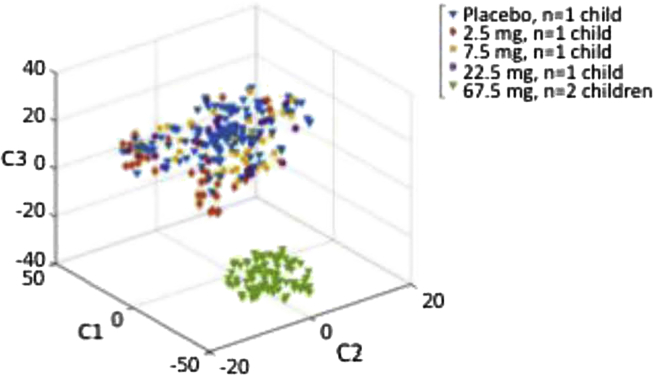
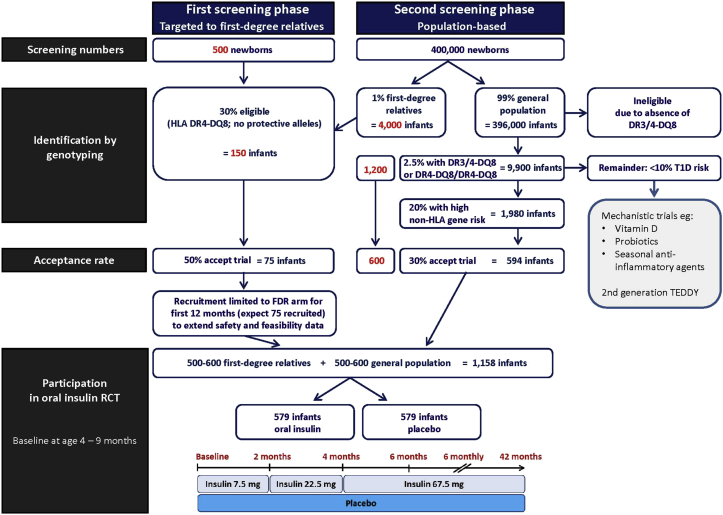
Results: Infants with a family history of type 1 diabetes (TRIGR, BABYDIET, TEDDY) and infants younger than age 3 months from the general population (FINDIA, TEDDY) were enrolled into these studies. All studies used HLA genotyping as part of their eligibility criteria. Predicted beta-cell autoimmunity risk in the eligible infants ranged from 3% (FINDIA, TEDDY general population) up to 12% (TRIGR, BABYDIET). Amongst eligible infants, participation was between 38% (TEDDY general population) and 97% (FINDIA). Outcomes, defined as multiple beta-cell autoantibodies, were consistent with predicted risks. We subsequently modeled recruitment into a randomized controlled trial (RCT) that could assess the efficacy of oral insulin treatment as adapted from the Pre-POINT pilot trial. The RCT would recruit infants with and without a first-degree family history of type 1 diabetes and be based on general population genetic risk testing. HLA genotyping and, for the general population, genotyping at additional type 1 diabetes susceptibility SNPs would be used to identify children with around 10% risk of beta-cell autoimmunity. The proposed RCT would have 80% power to detect a 50% reduction in multiple beta-cell autoantibodies by age 4 years at a two-tailed alpha of 0.05, and would randomize around 1160 infants to oral insulin or placebo arms in order to fulfill this. It is estimated that recruitment would require testing of between 400,000 and 500,000 newborns or infants.
Conclusion: It is timely and feasible to establish a platform for primary prevention trials for type 1 diabetes in Europe. This multi-site European infrastructure would perform RCTs, supply data coordination and biorepository, provide cohorts for mechanistic and observational studies, and increase awareness for autoimmune diabetes.
Keywords: Antigen-based immunotherapy; Beta-cell autoimmunity; Prevention; Type 1 diabetes.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
