

Influence of the short-axis cine acquisition protocol on the cardiac function evaluation: A reproducibility study
- PMID: 27069981
- PMCID: PMC4811847
- DOI: 10.1016/j.ejro.2016.03.003
Influence of the short-axis cine acquisition protocol on the cardiac function evaluation: A reproducibility study
Abstract
Purpose: To define the optimal cardiac short-axis cine acquisition protocol for the assessment of the left and rightventricular functions.
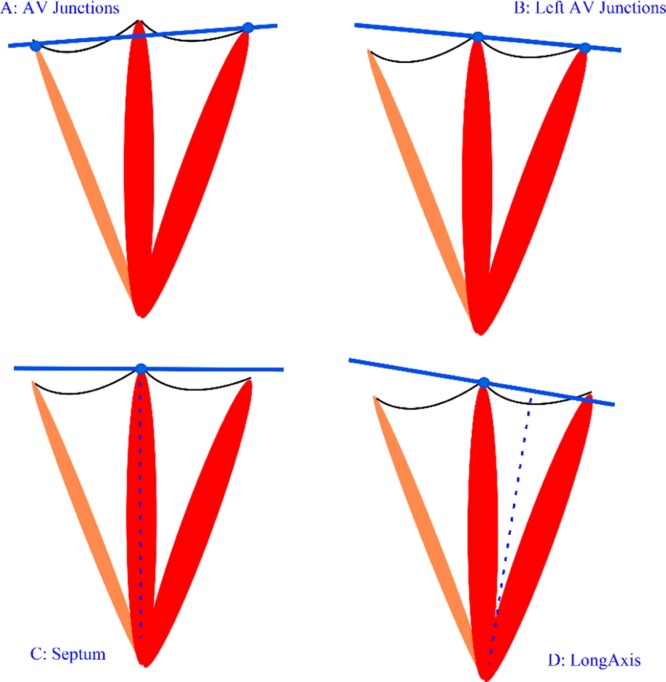
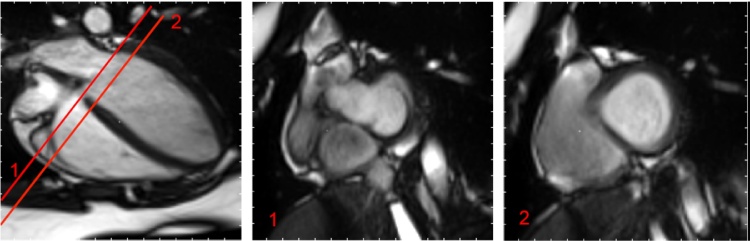
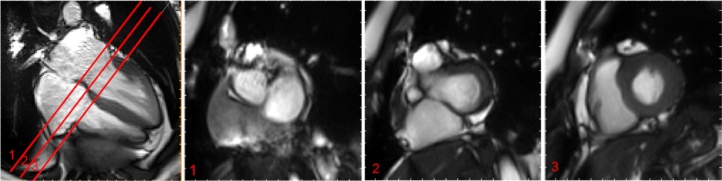
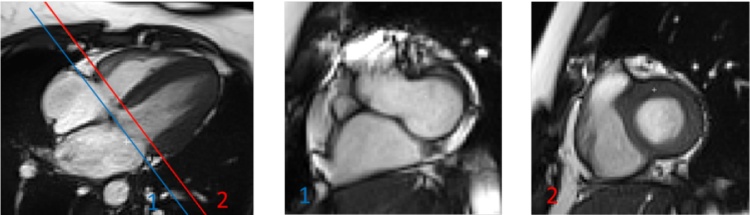
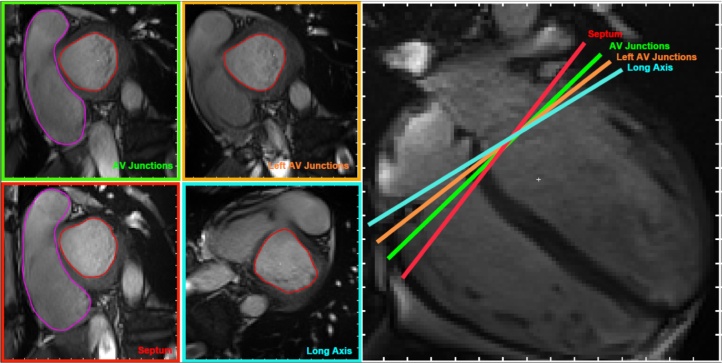
Materials and methods: 20 volunteers were recruited and breath-hold CINE images were acquired on a Siemens Prisma 3T MRI. Four short-axis acquisition planes were defined from the 4-chamber view. AV Junctions: short-axis slices parallel to the plane that cuts through the external right and left atrioventricular junctions. Left AV Junctions: short-axis slices parallel to the plane that cuts through both left atrioventricular junctions. Septum: short-axis slices perpendicular to the septum with one cutting through the septum junction. LongAxis: short-axis slices perpendicular to the long axis with one cutting through the septum junction. Intra and inter reproducibility was assessed using Bland-Altman coefficient of variation (CV) and Lin's concordance correlation coefficient (CCC). The influence of the protocol on the ejection fraction (EF) and stroke volume (SV) was quantified statistically using pair-wise CV and Pearson's correlation coefficient R (2).
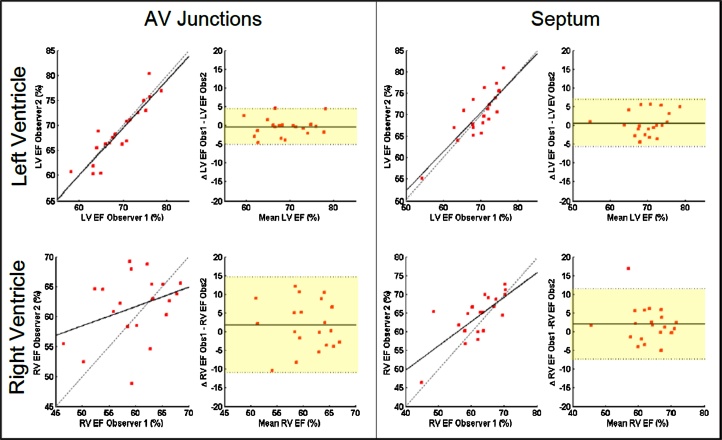
Results: All protocols led to high reproducibility for the LV EF (mean intra CV = 3.83%, mean inter CV = 4.81%, lowest CV = 4.20% (AV junctions) and highest CV = 5.24% (Left AV Junctions)). Reproducibility of the RV measurements was lower (mean intra CV = 7.84%, mean inter CV = 9.17%). Septum protocol led to significantly lower variability compared to the other 3 protocols for RV EF (CV = 7.62% (Septum), CV = 8.42% (Long Axis), CV = 9.54% (Left AV Junctions) and CV = 11.08% (AV Junctions) with Lin's CCC varying from 0.4 (AV Junctions) to 0.69 (Septum) for inter-observer reproducibility). No differences in group average for clinical parameters was found for both LV and RV clinical measurements. However, patient-specific RV EF evaluation is dependent on the chosen protocol (CV = 9.95%, R (2) = 0.52).
Conclusion: Based on the results of the study cine mode short-axis acquisitions should be planned perpendicular to the septum in order to guarantee optimal RV and LV measurements.
Keywords: Cine MRI; Left ventricle; Reproducibility study; Right ventricle; Short-axis acquisition.
Figures
References
-
- Grothues F., Smith G.C., Moon J.C., Bellenger N.G., Collins P., Klein H.U., Pennell D.J. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am. J. cardiol. 2002;90(1):29–34. - PubMed
-
- Myerson S.G., Bellenger N.G., Pennell D.J. Assessment of left ventricular mass by cardiovascular magnetic resonance. Hypertension. 2002;39(3):750–755. - PubMed
-
- Bellenger N.G., Francis J.M., Davies C.L., Coats A.J., Pennell D.J. Establishment and performance of a magnetic resonance cardiac function clinic. J. Cardiovasc. Magn. Reson. 2000;2(1):15–22. - PubMed
-
- Danilouchkine M.G., Westenberg J.J., de Roos A., Reiber J.H., Lelieveldt B.P. Operator induced variability in cardiovascular MR: left ventricular measurements and their reproducibility. J. Cardiovasc. Magn. Reson. 2005;7(2):447–457. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
