

Prevalence and Predictive Value of Dyspnea Ratings in Hospitalized Patients: Pilot Studies
- PMID: 27070144
- PMCID: PMC4829144
- DOI: 10.1371/journal.pone.0152601
Prevalence and Predictive Value of Dyspnea Ratings in Hospitalized Patients: Pilot Studies
Abstract
Background: Dyspnea (breathing discomfort) can be as powerfully aversive as pain, yet is not routinely assessed and documented in the clinical environment. Routine identification and documentation of dyspnea is the first step to improved symptom management and it may also identify patients at risk of negative clinical outcomes.
Objective: To estimate the prevalence of dyspnea and of dyspnea-associated risk among hospitalized patients.
Design: Two pilot prospective cohort studies.
Setting: Single academic medical center.
Patients: Consecutive patients admitted to four inpatient units: cardiology, hematology/oncology, medicine, and bariatric surgery.
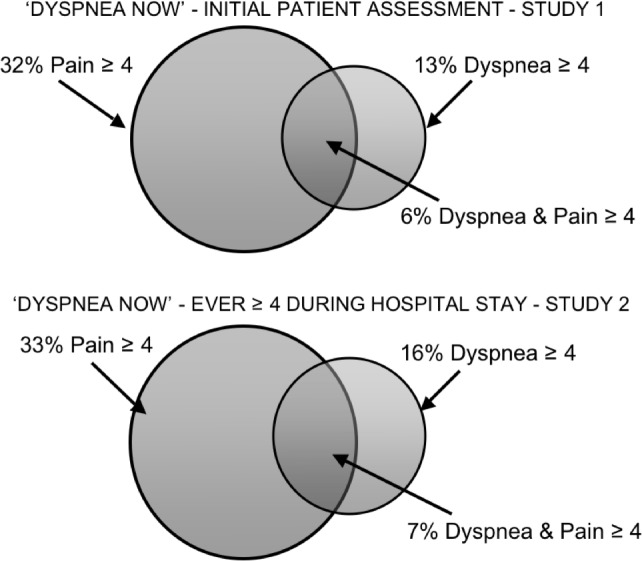
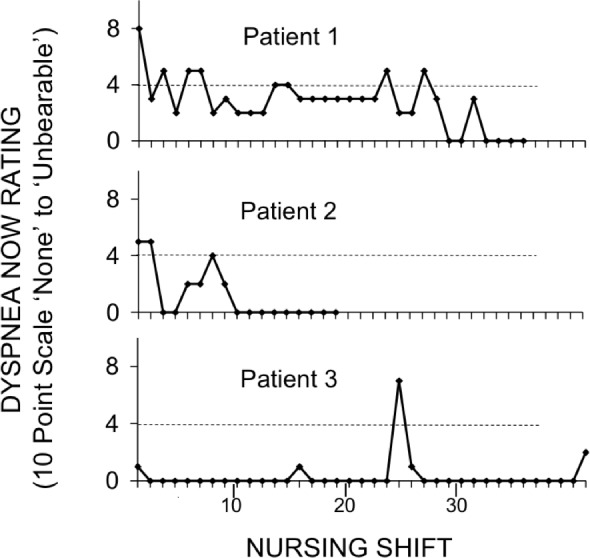
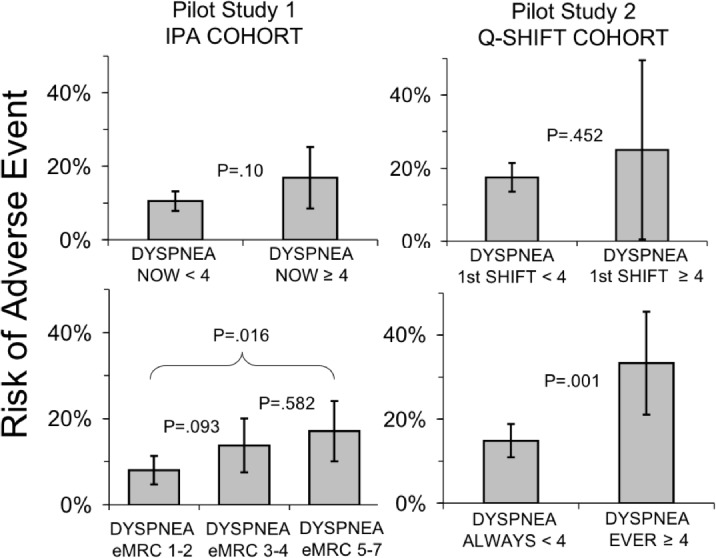
Measurements: In Study 1, nurses documented current and recent patient-reported dyspnea at the time of the Initial Patient Assessment in 581 inpatients. In Study 2, nurses documented current dyspnea at least once every nursing shift in 367 patients. We describe the prevalence of burdensome dyspnea, and compare it to pain. We also compared dyspnea ratings with a composite of adverse outcomes: 1) receipt of care from the hospital's rapid response system, 2) transfer to the intensive care unit, or 3) death in hospital. We defined burdensome dyspnea as a rating of 4 or more on a 10-point scale.
Results: Prevalence of burdensome current dyspnea upon admission (Study 1) was 13% (77 of 581, 95% CI 11%-16%). Prevalence of burdensome dyspnea at some time during the hospitalization (Study 2) was 16% (57 of 367, 95% CI 12%-20%). Dyspnea was associated with higher odds of a negative outcome.
Conclusions: In two pilot studies, we identified a significant symptom burden of dyspnea in hospitalized patients. Patients reporting dyspnea may benefit from a more careful focus on symptom management and may represent a population at greater risk for negative outcomes.
Conflict of interest statement
Figures
References
-
- O'Driscoll M, Corner J, Bailey C (1999) The experience of breathlessness in lung cancer. Eur J Cancer Care (Engl) 8: 37–43. - PubMed
-
- Thomas JR, von Gunten CF (2002) Clinical management of dyspnoea. Lancet Oncol 3: 223–228. - PubMed
-
- Shih FJ, Chu SH (1999) Comparisons of American-Chinese and Taiwanese patients' perceptions of dyspnea and helpful nursing actions during the intensive care unit transition from cardiac surgery. Heart Lung 28: 41–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
