

Prehospital traumatic cardiac arrest: Management and outcomes from the resuscitation outcomes consortium epistry-trauma and PROPHET registries
- PMID: 27070438
- PMCID: PMC4961534
- DOI: 10.1097/TA.0000000000001070
Prehospital traumatic cardiac arrest: Management and outcomes from the resuscitation outcomes consortium epistry-trauma and PROPHET registries
Abstract
Background: Traumatic arrests have historically had poor survival rates. Identifying salvageable patients and ideal management is challenging. We aimed to (1) describe the management and outcomes of prehospital traumatic arrests; (2) determine regional variation in survival; and (3) identify Advanced Life Support (ALS) procedures associated with survival.
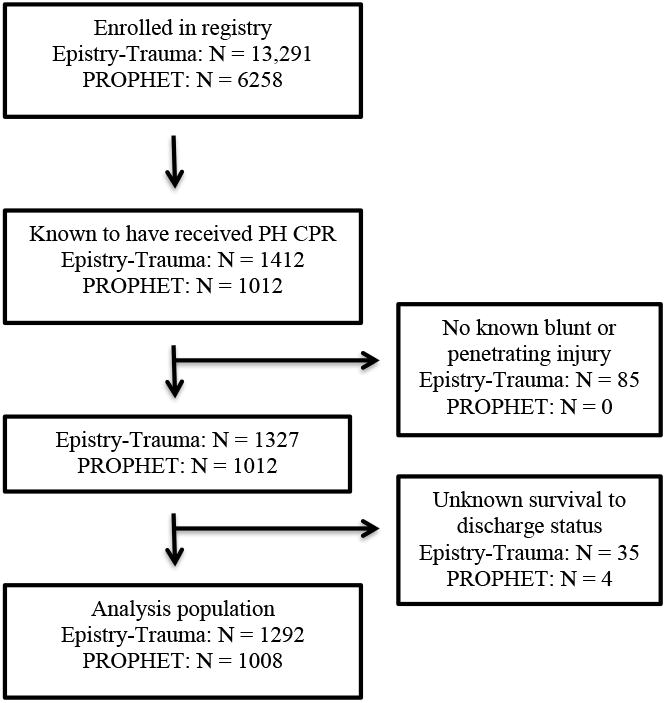
Methods: This was a secondary analysis of cases from the Resuscitation Outcomes Consortium Epistry-Trauma and Prospective Observational Prehospital and Hospital Registry for Trauma (PROPHET) registries. Patients were included if they had a blunt or penetrating injury and received cardiopulmonary resuscitation. Logistic regression analyses were used to determine the association between ALS procedures and survival.
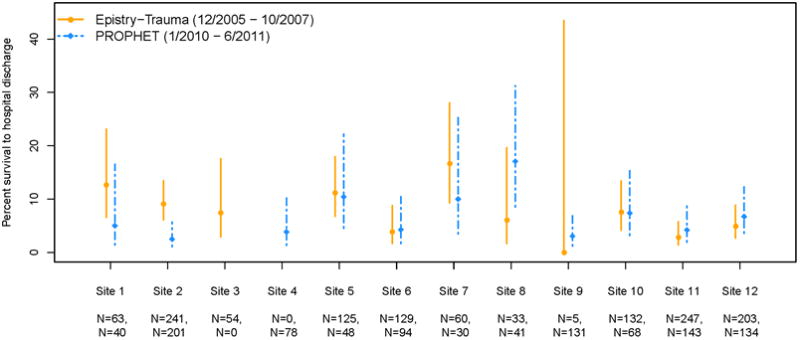
Results: We included 2,300 patients who were predominately young (Epistry mean [SD], 39 [20] years; PROPHET mean [SD], 40 [19] years), males (79%), injured by blunt trauma (Epistry, 68%; PROPHET, 67%), and treated by ALS paramedics (Epistry, 93%; PROPHET, 98%). A total of 145 patients (6.3%) survived to hospital discharge. More patients with blunt (Epistry, 8.3%; PROPHET, 6.5%) vs. penetrating injuries (Epistry, 4.6%; PROPHET, 2.7%) survived. Most survivors (81%) had vitals on emergency medical services arrival. Rates of survival varied significantly between the 12 study sites (p = 0.048) in the Epistry but not PROPHET (p = 0.14) registries.Patients in the PROPHET registry who received a supraglottic airway insertion or intubation experienced decreased odds of survival (adjusted OR, 0.27; 95% confidence interval, 0.08-0.93; and 0.37; 95% confidence interval, 0.17-0.78, respectively) compared to those receiving bag-mask ventilation. No other procedures were associated with survival.
Conclusions: Survival from traumatic arrest may be higher than expected, particularly in blunt trauma and patients with vitals on emergency medical services arrival. Although limited by confounding and statistical power, no ALS procedures were associated with increased odds of survival.
Level of evidence: Prognostic study, level IV.
Conflict of interest statement
Figures
References
-
- Millin MG, Galvagno SM, Khandker SR, Malki A, Bulger EM, Standards Clinical Practice Committee of the National Association of EMSP, Subcommittee on Emergency Services-Prehospital of the American College of Surgeons' Committee on Trauma. Withholding and termination of resuscitation of adult cardiopulmonary arrest secondary to trauma: resource document to the joint NAEMSP-ACSCOT position statements. J Trauma Acute Care Surg. 2013;75(3):459–67. - PubMed
-
- Tarmey N, Park C, Bartels O, Konig T, Mahoney P, Mellor A. Outcomes following military traumatic cardiorespiratory arrest: A prospective observational study. Resuscitation. 2011;82(9):1194–97. - PubMed
-
- Willis CD, Cameron PA, Bernard SA, Fitzgerald M. Cardiopulmonary resuscitation after traumatic cardiac arrest is not always futile. Injury. 2006;37(5):448–54. - PubMed
-
- Lockey D, Crewdson K, Davies G. Traumatic cardiac arrest: who are the survivors? Ann Emerg Med. 2006;48(3):240–4. - PubMed
-
- Pickens JJ, Copass MK, Bulger EM. Trauma Patients Receiving CPR: Predictors of Survival. The Journal of Trauma: Injury, Infection, and Critical Care. 2005;58(5):951–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
