

Extending resuscitative endovascular balloon occlusion of the aorta: Endovascular variable aortic control in a lethal model of hemorrhagic shock
- PMID: 27070441
- PMCID: PMC4961606
- DOI: 10.1097/TA.0000000000001075
Extending resuscitative endovascular balloon occlusion of the aorta: Endovascular variable aortic control in a lethal model of hemorrhagic shock
Abstract
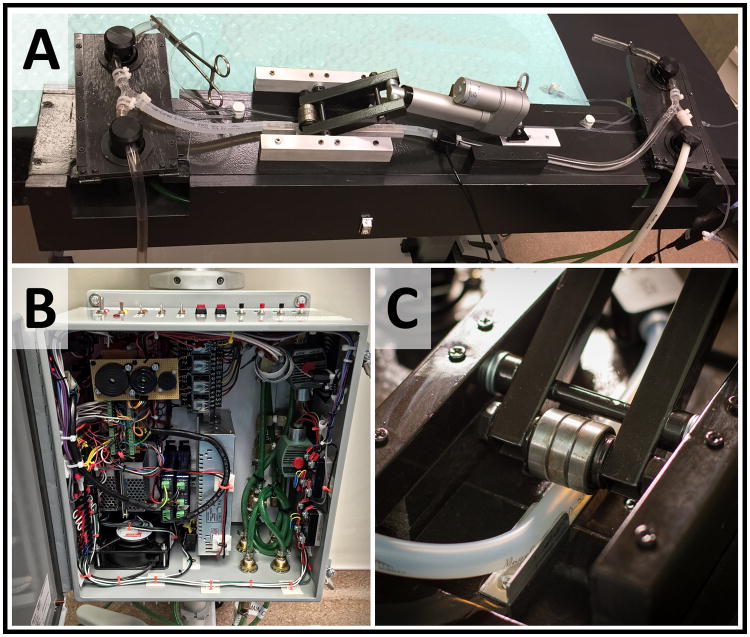
Background: The duration of use and efficacy of resuscitative endovascular balloon occlusion of the aorta (REBOA) is limited by distal ischemia. We developed a hybrid endovascular-extracorporeal circuit variable aortic control (VAC) device to extend REBOA duration in a lethal model of hemorrhagic shock to serve as an experimental surrogate to further the development of endovascular VAC (EVAC) technologies.
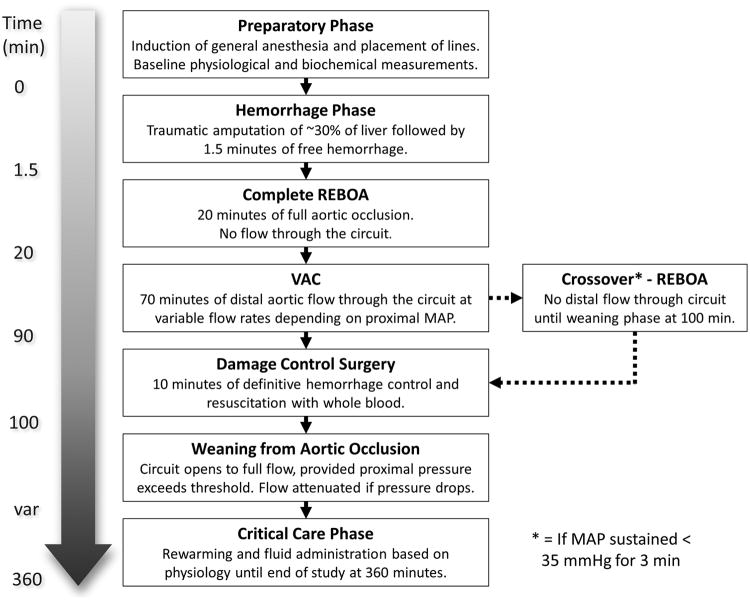
Methods: Nine Yorkshire-cross swine were anesthetized, instrumented, splenectomized, and subjected to 30% liver amputation. Following a short period of uncontrolled hemorrhage, REBOA was instituted for 20 minutes. Automated variable occlusion in response to changes in proximal mean arterial pressure was applied for the remaining 70 minutes of the intervention phase using the automated extracorporeal circuit. Damage-control surgery and whole blood resuscitation then occurred, and the animals were monitored for a total of 6 hours.
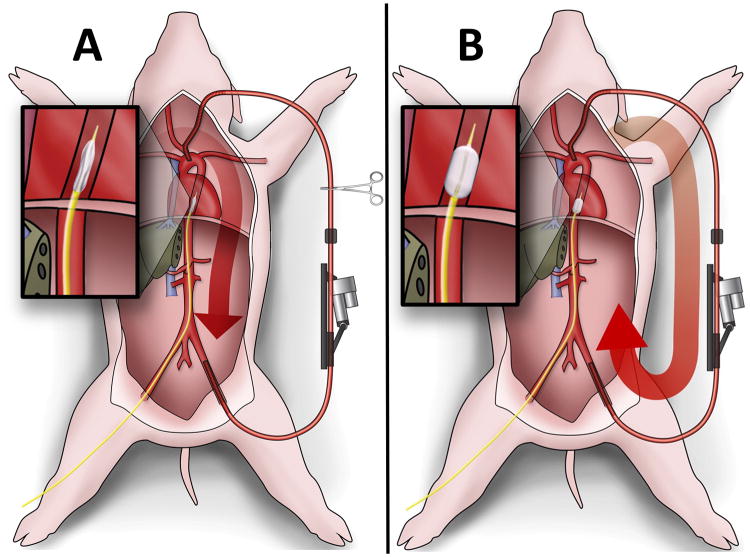
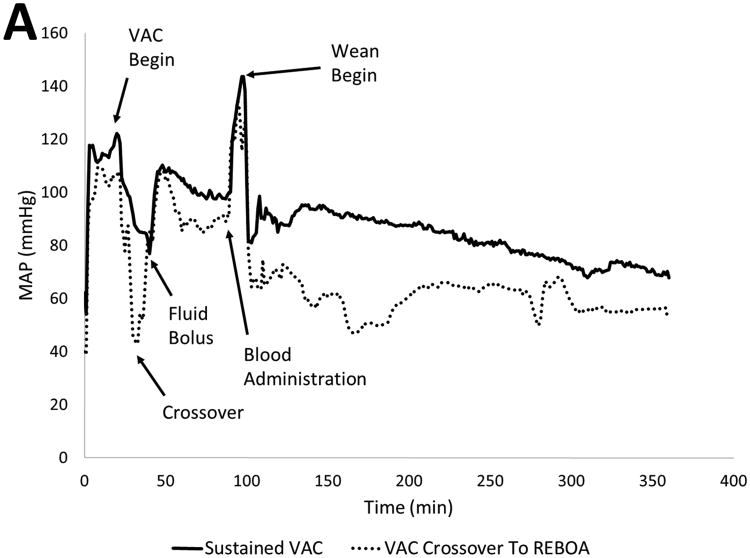
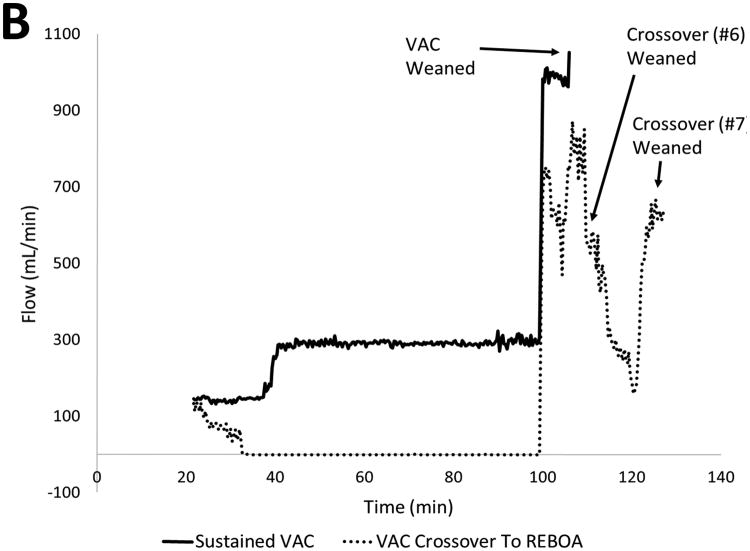
Results: Seven animals survived the initial surgical preparation. After 20 minutes of complete REBOA, regulated flow was initiated through the extracorporeal circuit to simulate VAC and provide perfusion to distal tissue beds during the 90-minute intervention phase. Two animals required circuit occlusion for salvage, while five animals tolerated sustained, escalating restoration of distal blood flow before surgical hemorrhage control. Animals tolerating distal flow had preserved renal function, maintained proximal blood pressure, and rapidly weaned from complete REBOA.
Conclusion: We combined a novel automated, extracorporeal circuit with complete REBOA to achieve EVAC in a swine model of uncontrolled hemorrhage. Our approach regulated proximal aortic pressure, alleviated supranormal values above the balloon, and provided controlled distal aortic perfusion that reduced ischemia without inducing intolerable bleeding. This experimental model serves as a temporary surrogate to guide future EVAC catheter designs that may provide transformational approaches to hemorrhagic shock.
Figures
Similar articles
-
Endovascular variable aortic control (EVAC) versus resuscitative endovascular balloon occlusion of the aorta (REBOA) in a swine model of hemorrhage and ischemia reperfusion injury.J Trauma Acute Care Surg. 2018 Sep;85(3):519-526. doi: 10.1097/TA.0000000000002008. J Trauma Acute Care Surg. 2018. PMID: 30142105
-
Incremental balloon deflation following complete resuscitative endovascular balloon occlusion of the aorta results in steep inflection of flow and rapid reperfusion in a large animal model of hemorrhagic shock.J Trauma Acute Care Surg. 2017 Jul;83(1):139-143. doi: 10.1097/TA.0000000000001502. J Trauma Acute Care Surg. 2017. PMID: 28632583 Free PMC article.
-
Partial Resuscitative Endovascular Balloon Occlusion of the Aorta in Swine Model of Hemorrhagic Shock.J Am Coll Surg. 2016 Aug;223(2):359-68. doi: 10.1016/j.jamcollsurg.2016.04.037. Epub 2016 Apr 29. J Am Coll Surg. 2016. PMID: 27138649
-
Partial Resuscitative Endovascular Balloon Occlusion of the Aorta: A Systematic Review of the Preclinical and Clinical Literature.J Surg Res. 2021 Jun;262:101-114. doi: 10.1016/j.jss.2020.12.054. Epub 2021 Feb 6. J Surg Res. 2021. PMID: 33561721
-
[Resuscitative endovascular balloon occlusion of the aorta (REBOA) : Current aspects of material, indications and limits: an overview].Chirurg. 2020 Nov;91(11):934-942. doi: 10.1007/s00104-020-01180-0. Chirurg. 2020. PMID: 32514942 Free PMC article. Review. German.
Cited by
-
Complete and Partial Aortic Occlusion for the Treatment of Hemorrhagic Shock in Swine.J Vis Exp. 2018 Aug 24;(138):58284. doi: 10.3791/58284. J Vis Exp. 2018. PMID: 30199035 Free PMC article.
-
Cerebral haemodynamics and intracranial pressure during haemorrhagic shock and resuscitation with total endovascular balloon occlusion of the aorta in an animal model.Eur J Trauma Emerg Surg. 2024 Dec;50(6):3069-3082. doi: 10.1007/s00068-024-02646-0. Epub 2024 Oct 25. Eur J Trauma Emerg Surg. 2024. PMID: 39453469 Free PMC article.
-
Validation of a miniaturized handheld arterial pressure monitor for guiding full and partial REBOA use during resuscitation.Eur J Trauma Emerg Surg. 2023 Apr;49(2):795-801. doi: 10.1007/s00068-022-02121-8. Epub 2022 Oct 23. Eur J Trauma Emerg Surg. 2023. PMID: 36273349
-
Automated Partial Versus Complete Resuscitative Endovascular Balloon Occlusion of the Aorta for the Management of Hemorrhagic Shock in a Pig Model of Polytrauma: a Randomized Controlled Pilot Study.Mil Med. 2020 Dec 30;185(11-12):e1923-e1930. doi: 10.1093/milmed/usaa217. Mil Med. 2020. PMID: 32830262 Free PMC article.
-
A scoping review of cognitive load assessment tools suitable for clinicians performing REBOA.Scand J Trauma Resusc Emerg Med. 2025 Jul 9;33(1):121. doi: 10.1186/s13049-025-01408-0. Scand J Trauma Resusc Emerg Med. 2025. PMID: 40635058 Free PMC article.
References
-
- Stannard A, Eliason JL, Rasmussen TE. Resuscitative endovascular balloon occlusion of the aorta (REBOA) as an adjunct for hemorrhagic shock. J Trauma Acute Care Surg. 2011;71(6):1869–72. - PubMed
-
- Brenner M, Moore L, Dubose J, Tyson G, McNutt M, Albarado R, Holcomb J, Scalea T, Rasmussen T. A clinical series of resuscitative endovascular balloon occlusion of the aorta for hemorrhage control and resuscitation. J Trauma. 2013;75(3):506–11. - PubMed
-
- Saito N, Matsumoto H, Yagi T, Hara Y, Hayashida K, Motomura T, Mashiko K, Iida H, Yokota H, Wagatsuma Y. Evaluation of the safety and feasibility of resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2015;78(5):897–904. - PubMed
-
- Matsuoka S, Uchiyama K, Shima H, Ohishi S, Nojiri Y, Ogata H. Temporary percutaneous aortic balloon occlusion to enhance fluid resuscitation prior to definitive embolization of post-traumatic liver hemorrhage. Cardiovasc Intervent Radiol. 2001;24(4):274–6. - PubMed
-
- Biffl WL, Fox CJ, Moore EE. The role of REBOA in the control of exsanguinating torso hemorrhage. J Trauma Acute Care Surg. 2015;78(5):1054–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
