

A Stochastic Individual-Based Model of the Progression of Atrial Fibrillation in Individuals and Populations
- PMID: 27070920
- PMCID: PMC4829251
- DOI: 10.1371/journal.pone.0152349
A Stochastic Individual-Based Model of the Progression of Atrial Fibrillation in Individuals and Populations
Abstract
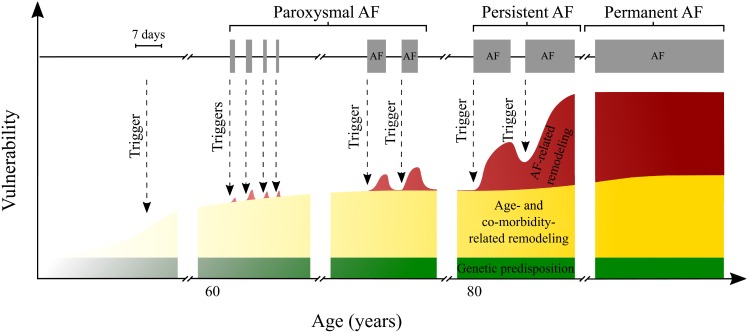
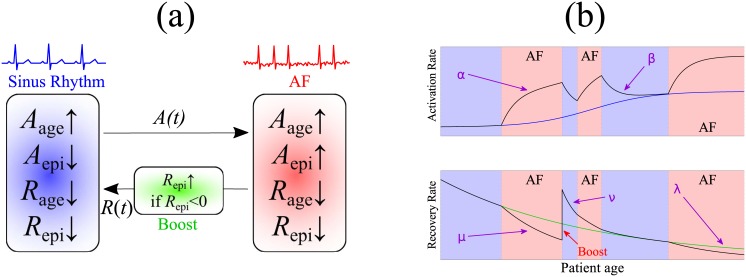
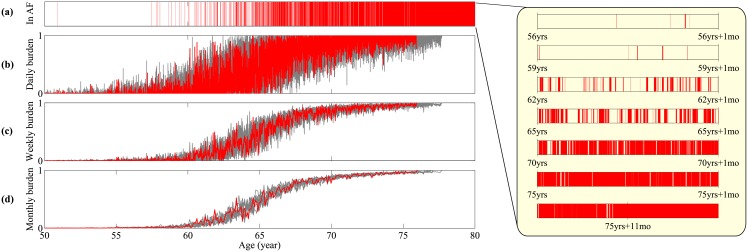
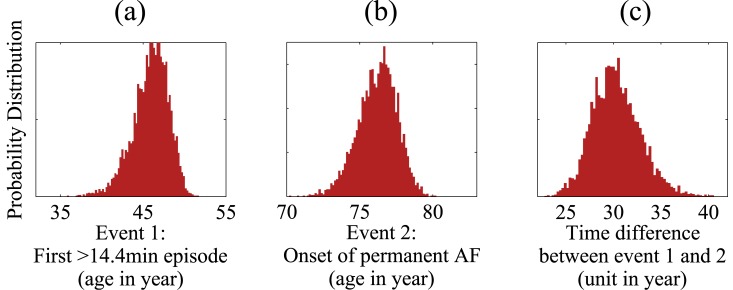
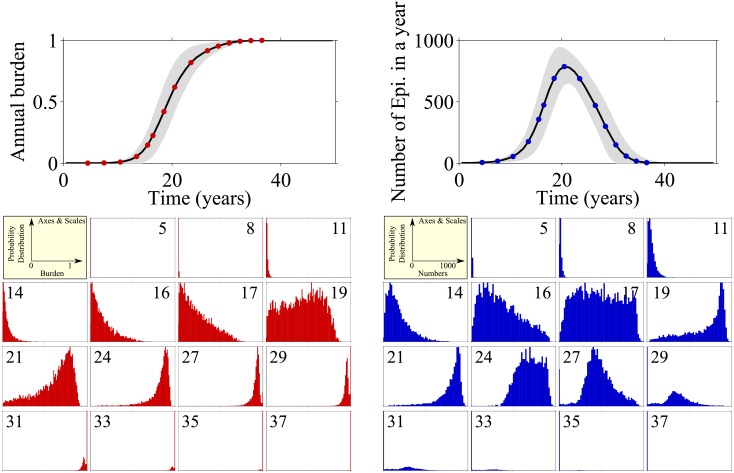
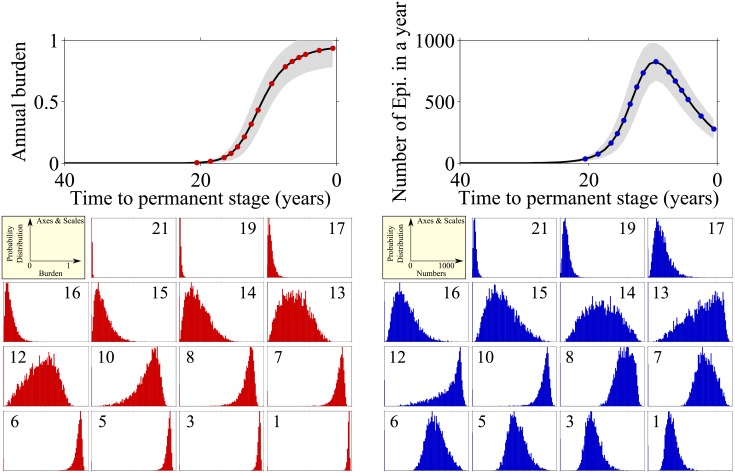
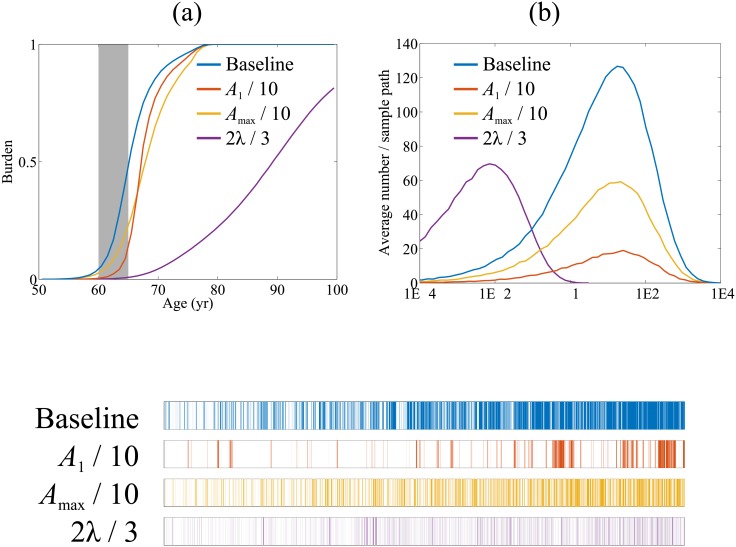
Models that represent the mechanisms that initiate and sustain atrial fibrillation (AF) in the heart are computationally expensive to simulate and therefore only capture short time scales of a few heart beats. It is therefore difficult to embed biophysical mechanisms into both policy-level disease models, which consider populations of patients over multiple decades, and guidelines that recommend treatment strategies for patients. The aim of this study is to link these modelling paradigms using a stylised population-level model that both represents AF progression over a long time-scale and retains a description of biophysical mechanisms. We develop a non-Markovian binary switching model incorporating three different aspects of AF progression: genetic disposition, disease/age related remodelling, and AF-related remodelling. This approach allows us to simulate individual AF episodes as well as the natural progression of AF in patients over a period of decades. Model parameters are derived, where possible, from the literature, and the model development has highlighted a need for quantitative data that describe the progression of AF in population of patients. The model produces time series data of AF episodes over the lifetimes of simulated patients. These are analysed to quantitatively describe progression of AF in terms of several underlying parameters. Overall, the model has potential to link mechanisms of AF to progression, and to be used as a tool to study clinical markers of AF or as training data for AF classification algorithms.
Conflict of interest statement
Figures
References
-
- National Collaborating Centre for Chronic Conditions. Atrial Fibrillation: National clinical guideline for management in primary and secondary care. Royal College of Physicians,; 2006. CG36 Available from: http://guidance.nice.org.uk/CG36. - PubMed
-
- National Clinical Guideline Centre. Atrial fibrillation: the management of atrial fibrillation. National Institute for Health and Care Excellence; 2014. CG180 ISBN 978-1-4731-0603-1. Available from: https://www.nice.org.uk/guidance/cg180.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
