

Long-Term Renal Outcomes after Cisplatin Treatment
- PMID: 27073199
- PMCID: PMC4934839
- DOI: 10.2215/CJN.08070715
Long-Term Renal Outcomes after Cisplatin Treatment
Abstract
Background and objectives: Nephrotoxicity remains the dose-limiting side effect of cisplatin, an effective chemotherapeutic agent with applications across diverse tumor types. This study presents data on renal outcomes across multiple tumor types in 821 adults. We report on incidence of AKI, initial and long-term changes in eGFR after cisplatin, and relationships between cumulative dose, initial eGFR, age, sex, and long-term renal function.
Design, setting, participants, & measurements: This was a retrospective study of adult patients treated with cisplatin from January 1, 2000 to September 21, 2011 who had survived ≥5 years after initial dose. The Modification of Diet in Renal Disease equation was used to calculate eGFR. AKI was defined as an increase from the baseline creatinine of >25% within 30 days after the first cycle of cisplatin. Chi-squared tests were done to evaluate the relationships between categorical or ordinal variables; ANOVAs or t tests were used to evaluate continuous or categorical variables. Changes in eGFR over time were evaluated in a growth curve model.
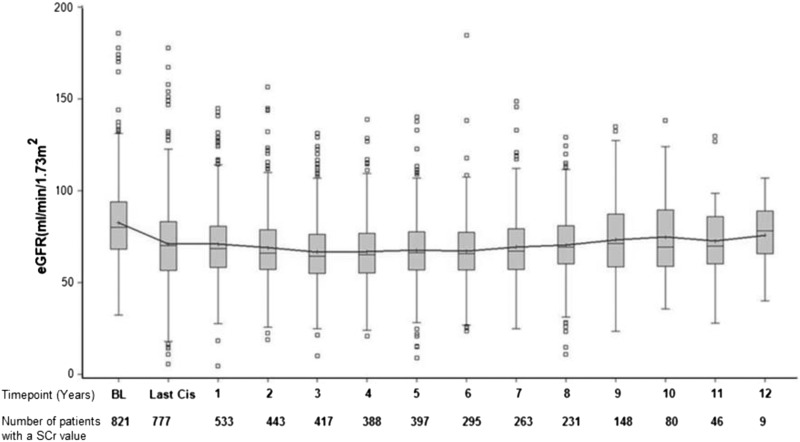
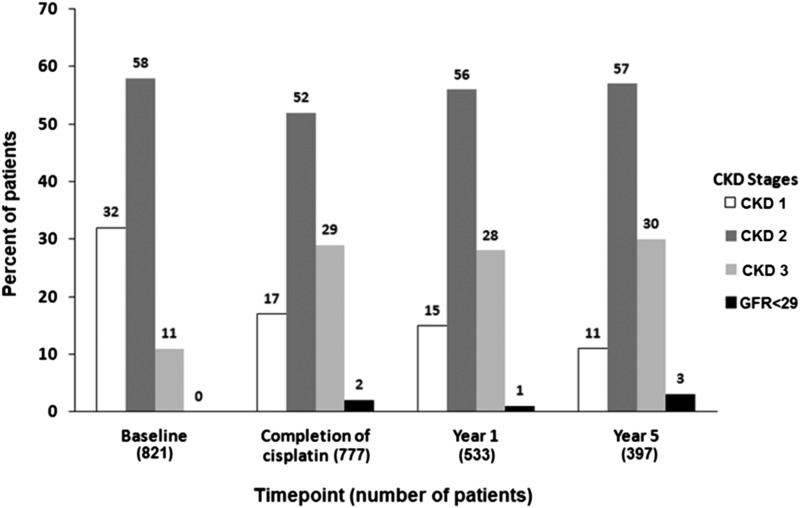
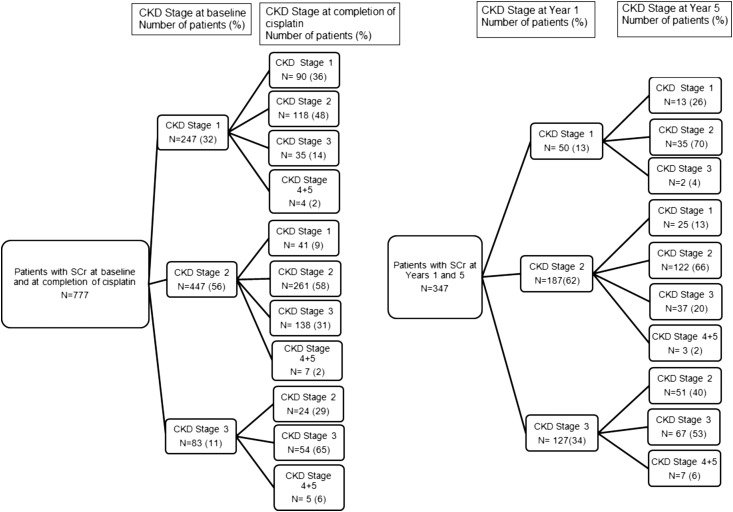
Results: Mean follow-up was 6 years (25th and 75th percentiles, 4 and 9 years). AKI occurred in 31.5% of patients, with a median initial decline in eGFR of 10 ml/min per 1.73 m(2) (25th and 75th percentiles, -41.5 and -23.3 ml/min per 1.73 m(2)). At any time point after the first cycle of cisplatin, <3% of patients progressed to eGFR<29 ml/min per 1.73 m(2), and none were known to be on dialysis. Age was associated with a higher risk for AKI after cisplatin. Compared with age <25 years old, the odds ratios for AKI versus no AKI are 1.22 for >26-44 years old (95% confidence interval [95% CI], 0.60 to 2.4), 1.54 for >45-65 years old (95% CI, 0.78 to 3), and 2.96 for >66 years old (95% CI, 1.4 to 6.1). The lowest dose categories of cisplatin (≤100 and 101-250 mg/m(2)) are associated with increases in eGFR (P=0.06 and P=0.02, respectively) compared with the highest dose category (>701 mg/m(2)).
Conclusions: This is the largest study of adult patients with cancer who received cisplatin for treatment across multiple tumor types. Most patients experience small but permanent declines in eGFR, but none progressed to ESRD requiring hemodialysis.
Keywords: Acute Kidney Injury; Follow-Up Studies; Humans; chronic kidney failure; cisplatin; cisplatin nephrotoxicity; creatinine; glomerular filtration rate; nephrotoxicity; renal dialysis.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Osanto S, Bukman A, Van Hoek F, Sterk PJ, De Laat JA, Hermans J: Long-term effects of chemotherapy in patients with testicular cancer. J Clin Oncol 10: 574–579, 1992 - PubMed
-
- Rosell R, Lord RV, Taron M, Reguart N: DNA repair and cisplatin resistance in non-small-cell lung cancer. Lung Cancer 38: 217–227, 2002 - PubMed
-
- Meyer KB, Madias NE: Cisplatin nephrotoxicity. Miner Electrolyte Metab 20: 201–213, 1994 - PubMed
-
- Taguchi T, Nazneen A, Abid MR, Razzaque MS: Cisplatin-associated nephrotoxicity and pathological events. Contrib Nephrol 148: 107–121, 2005 - PubMed
-
- Sastry J, Kellie SJ: Severe neurotoxicity, ototoxicity and nephrotoxicity following high-dose cisplatin and amifostine. Pediatr Hematol Oncol 22: 441–445, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
