

Validity of breast-specific gamma imaging for Breast Imaging Reporting and Data System 4 lesions on mammography and/or ultrasound
- PMID: 27073789
- PMCID: PMC4826981
- DOI: 10.4174/astr.2016.90.4.194
Validity of breast-specific gamma imaging for Breast Imaging Reporting and Data System 4 lesions on mammography and/or ultrasound
Abstract
Purpose: The purpose of this study was to assess the breast-specific gamma imaging (BSGI) in Breast Imaging Reporting and Data System (BI-RADS) 4 lesions on mammography and/or ultrasound.
Methods: We performed a retrospective review of 162 patients who underwent BSGI in BI-RADS 4 lesions on mammography and/or ultrasound.
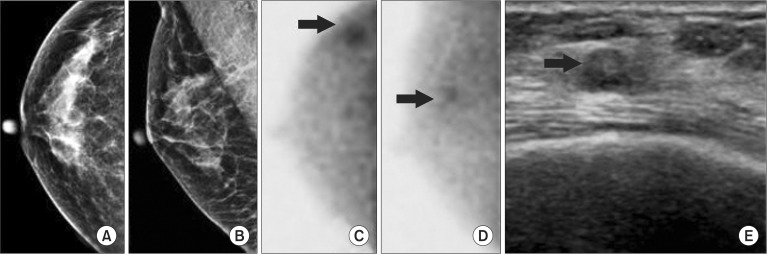
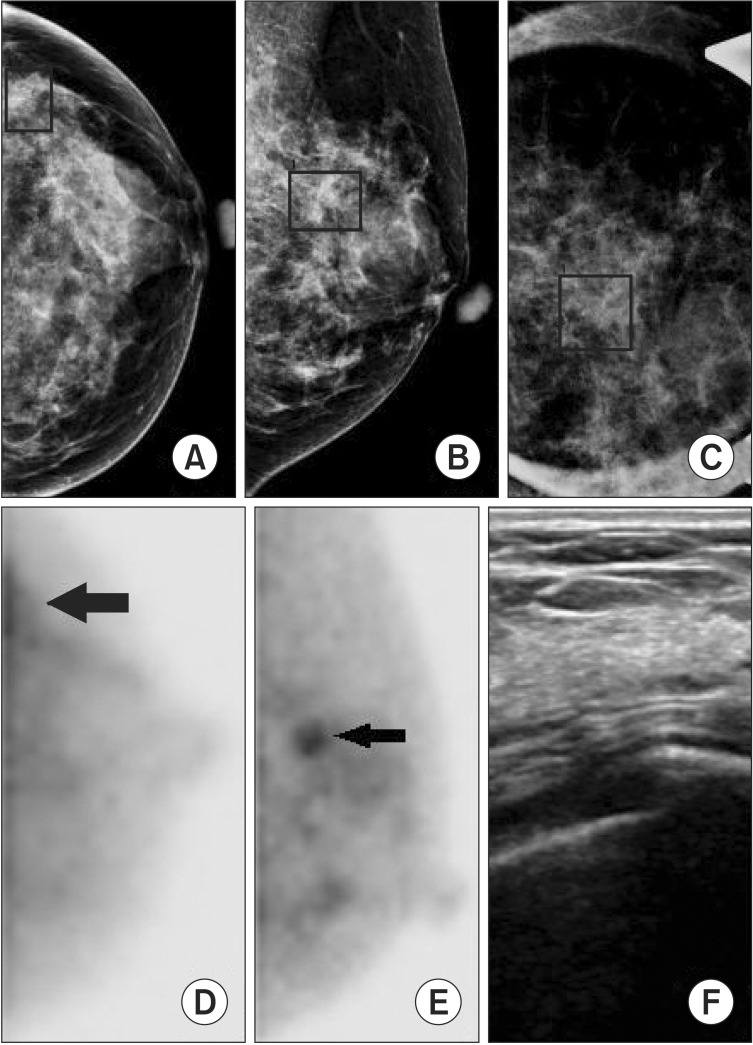
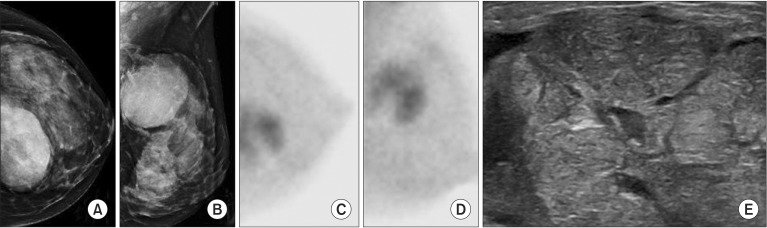
Results: Of the 162 breast lesions, 66 were malignant tumors and 96 were benign tumors. Sensitivity and specificity of BSGI were 90.9% and 78.1%, and positive predictive value and negative predictive value were 74.1% and 92.6%. The sensitivity or specificity of mammography and ultrasound were 74.2% and 56.3% and 87.9% and 19.8%, respectively. The sensitivity and specificity of BSGI for breast lesions ≤1 cm were 88.0% and 86.8%, while the values of beast lesions >1 cm were 92.7% and 61.5%. The sensitivity or specificity of BSGI and mammography for patients with dense breasts were 92.0% and 81.3% and 72.0% and 50.0%, respectively. 26 patients showed neither a nodule nor microcalcification on ultrasound, but showed suspicious calcification on mammography. The sensitivity and specificity of BSGI with microcalcification only lesion were 75.0% and 94.4%.
Conclusion: This study demonstrated that BSGI had shown high sensitivity and specificity, as well as positive and negative predictive values in BI-RADS 4 lesions on ultrasound and/or mammography. BSGI showed excellent results in dense breasts, in lesions that are less than 1 cm in size and lesions with suspicious microcalcification only.
Keywords: Breast neoplasms; Breast specific gamma imaging; Mammography; Ultrasonography.
Conflict of interest statement
Figures
References
-
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. 2002;225:165–175. - PubMed
-
- Rosenberg RD, Hunt WC, Williamson MR, Gilliland FD, Wiest PW, Kelsey CA, et al. Effects of age, breast density, ethnicity, and estrogen replacement therapy on screening mammographic sensitivity and cancer stage at diagnosis: review of 183,134 screening mammograms in Albuquerque, New Mexico. Radiology. 1998;209:511–518. - PubMed
-
- Berg WA, Gutierrez L, NessAiver MS, Carter WB, Bhargavan M, Lewis RS, et al. Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology. 2004;233:830–849. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
