

Commissioning and initial experience with the first clinical gantry-mounted proton therapy system
- PMID: 27074470
- PMCID: PMC5874960
- DOI: 10.1120/jacmp.v17i2.5868
Commissioning and initial experience with the first clinical gantry-mounted proton therapy system
Abstract
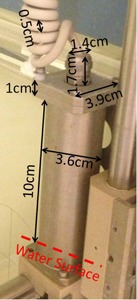
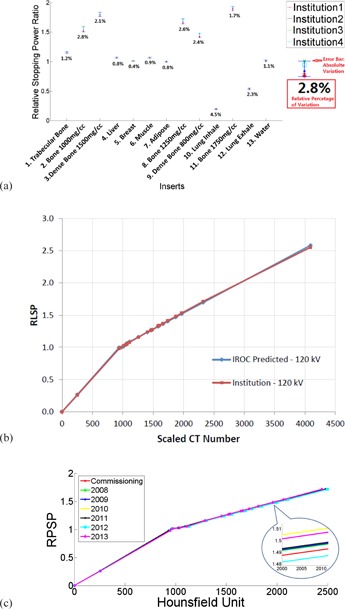
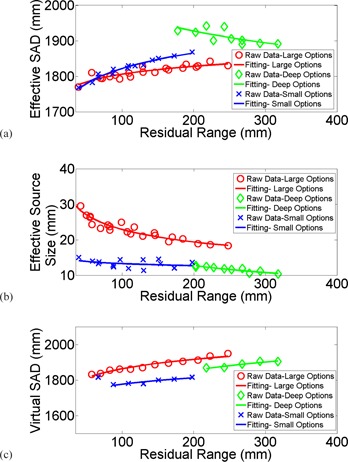
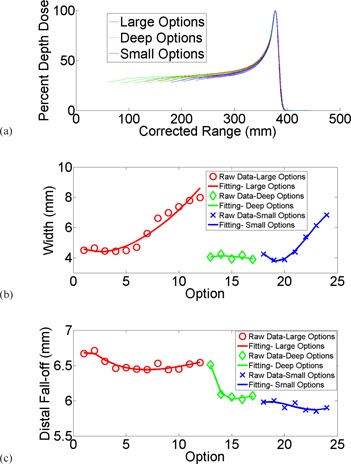
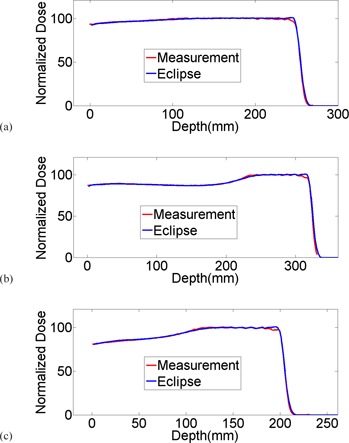
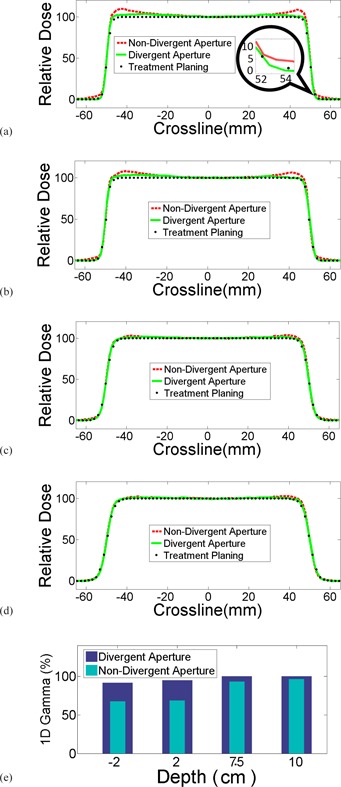
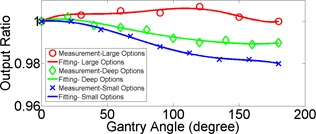
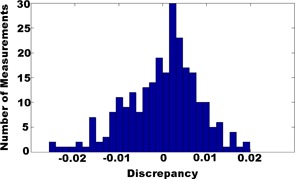
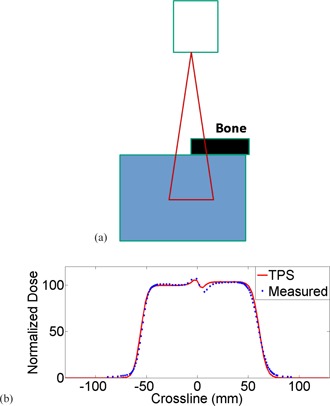
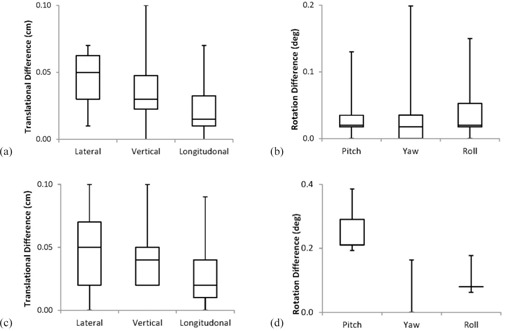
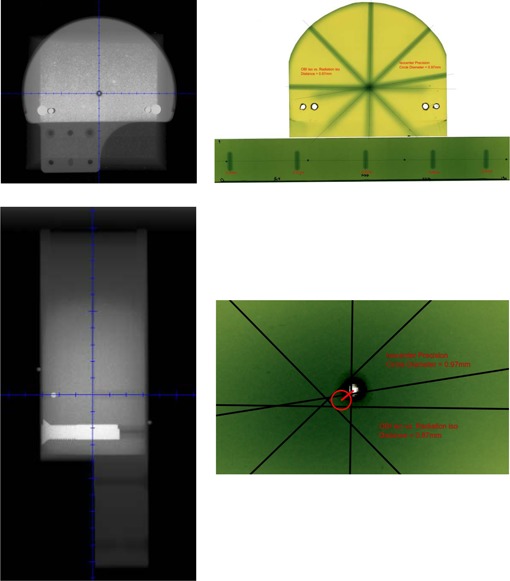
The purpose of this study is to describe the comprehensive commissioning process and initial clinical experience of the Mevion S250 proton therapy system, a gantry-mounted, single-room proton therapy platform clinically implemented in the S. Lee Kling Proton Therapy Center at Barnes-Jewish Hospital in St. Louis, MO, USA. The Mevion S250 system integrates a compact synchrocyclotron with a C-inner gantry, an image guidance system and a 6D robotic couch into a beam delivery platform. We present our commissioning process and initial clinical experience, including i) CT calibration; ii) beam data acquisition and machine characteristics; iii) dosimetric commissioning of the treatment planning system; iv) validation through the Imaging and Radiation Oncology Core credentialing process, including irradiations on the spine, prostate, brain, and lung phantoms; v) evaluation of localization accuracy of the image guidance system; and vi) initial clinical experience. Clinically, the system operates well and has provided an excellent platform for the treatment of diseases with protons.
Figures
References
-
- Levy RP, Blakely EA, Chu WT, et al. The current status and future directions of heavy charged particle therapy in medicine. AIP Conference Proceedings. 2009;1099(1):410–25. doi:10.1063/1.3120064
-
- St Clair WH, Adams JA, Bues M, et al. Advantage of protons compared to conventional X‐ray or IMRT in the treatment of a pediatric patient with medulloblastoma. Int J Radiat Oncol Biol Phys. 2004;58(3):727–34. - PubMed
-
- Schaffner B and Pedroni E. The precision of proton range calculations in proton radiotherapy treatment planning: experimental verification of the relation between CT‐HU and proton stopping power. Phys Med Biol. 1998;43(6):1579–92. - PubMed
-
- Schneider U, Pedroni E, Lomax A. The calibration of CT Hounsfield units for radiotherapy treatment planning. Phys Med Biol. 1996;41(1):111–24. - PubMed
-
- Pemler P, Schneider U, Besserer J. [Evaluation of the electron density phantom CIRS Model 62] [in German]. Z Med Phys. 2001;11(1):25–32. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
