

Risk factors for future repeat abdominal surgery
- PMID: 27074725
- PMCID: PMC5009167
- DOI: 10.1007/s00423-016-1414-3
Risk factors for future repeat abdominal surgery
Abstract
Purpose: Today, 40 to 66 % of elective procedures in abdominal surgery are reoperations. Reoperations show increased operative time and risk for intraoperative and postoperative complications, mainly due to the need to perform adhesiolysis. It is important to understand which patients will require repeat surgery for optimal utilization and implementation of anti-adhesive strategies. Our aim is to assess the incidence and identify risk factors for repeat abdominal surgery.
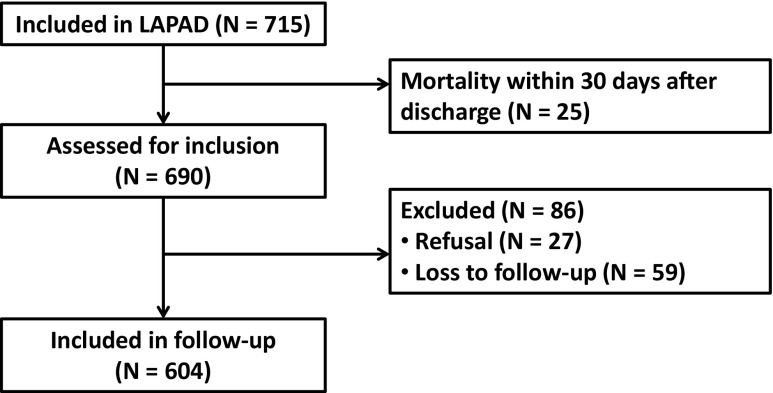
Methods: This is the long-term follow-up of a prospective cohort study (Laparotomy or Laparoscopy and Adhesions (LAPAD) study; clinicaltrials.gov NCT01236625). Patients undergoing elective abdominal surgery were included. Primary outcome was future repeat abdominal surgery and was defined as any operation where the peritoneal cavity is reopened. Multivariable logistic regression analysis was used to identify risk factors.
Results: Six hundred four (88 %) out of 715 patients were included; median duration of follow-up was 46 months. One hundred sixty (27 %) patients required repeat abdominal surgery and underwent a total of 234 operations. The indication for repeat surgery was malignant disease recurrence in 49 (21 %), incisional hernia in 41 (18 %), and indications unrelated to the index surgery in 58 (25 %) operations. Older age (OR 0.98; p 0.002) and esophageal malignancy (OR 0.21; p 0.034) significantly reduced the risk of undergoing repeat abdominal surgery. Female sex (OR 1.53; p 0.046) and hepatic malignancy as indication for surgery (OR 2.08; p 0.049) significantly increased the risk of requiring repeat abdominal surgery.
Conclusions: One in four patients will require repeat surgery within 4 years after elective abdominal surgery. Lower age, female sex, and hepatic malignancy are significant risk factors for requiring repeat abdominal surgery.
Keywords: Abdominal adhesions; Abdominal surgery; Postoperative complications; Risk factors.
Conflict of interest statement
Compliance with ethical standards All procedures performed in studies involving human participants were in accordance with the ethical standards of the medical ethical committee of the Radboud University Medical Center (registration number 2013/097) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Funding No funding was obtained for this study. Conflicts of interest The authors declare that they have no conflict of interest.
Figures

References
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
