

Real-Time Risk Prediction on the Wards: A Feasibility Study
- PMID: 27075140
- PMCID: PMC4949091
- DOI: 10.1097/CCM.0000000000001716
Real-Time Risk Prediction on the Wards: A Feasibility Study
Abstract
Objective: Failure to detect clinical deterioration in the hospital is common and associated with poor patient outcomes and increased healthcare costs. Our objective was to evaluate the feasibility and accuracy of real-time risk stratification using the electronic Cardiac Arrest Risk Triage score, an electronic health record-based early warning score.
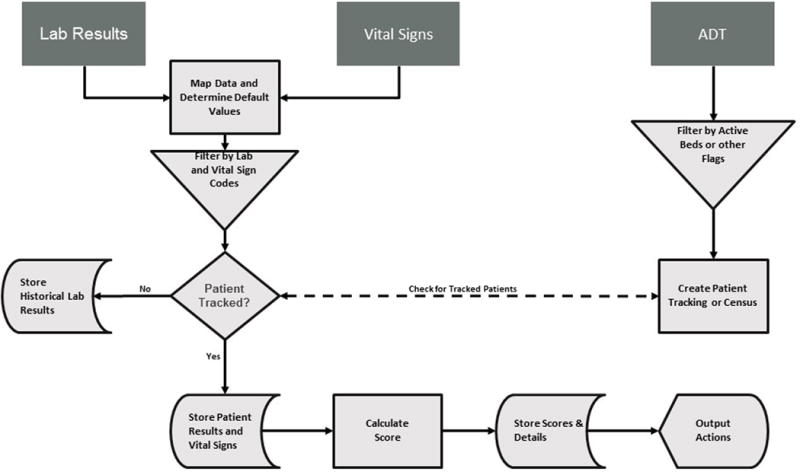
Design: We conducted a prospective black-box validation study. Data were transmitted via HL7 feed in real time to an integration engine and database server wherein the scores were calculated and stored without visualization for clinical providers. The high-risk threshold was set a priori. Timing and sensitivity of electronic Cardiac Arrest Risk Triage score activation were compared with standard-of-care Rapid Response Team activation for patients who experienced a ward cardiac arrest or ICU transfer.
Setting: Three general care wards at an academic medical center.
Patients: A total of 3,889 adult inpatients.
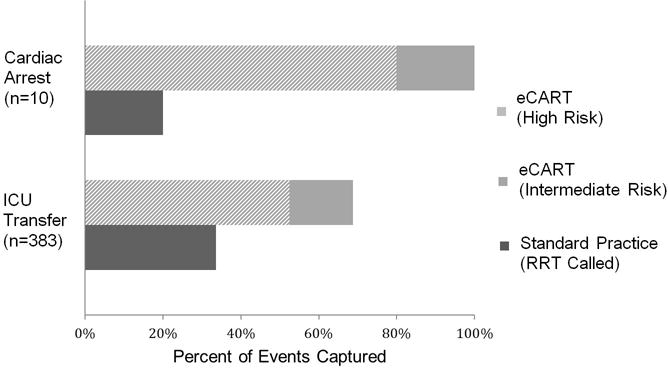
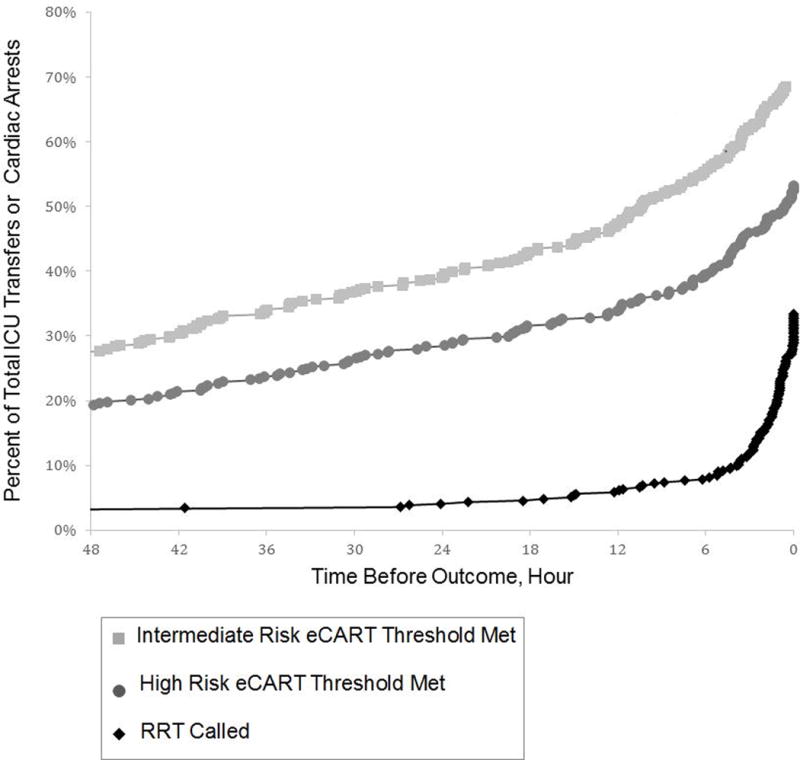
Measurements and main results: The system generated 5,925 segments during 5,751 admissions. The area under the receiver operating characteristic curve for electronic Cardiac Arrest Risk Triage score was 0.88 for cardiac arrest and 0.80 for ICU transfer, consistent with previously published derivation results. During the study period, eight of 10 patients with a cardiac arrest had high-risk electronic Cardiac Arrest Risk Triage scores, whereas the Rapid Response Team was activated on two of these patients (p < 0.05). Furthermore, electronic Cardiac Arrest Risk Triage score identified 52% (n = 201) of the ICU transfers compared with 34% (n = 129) by the current system (p < 0.001). Patients met the high-risk electronic Cardiac Arrest Risk Triage score threshold a median of 30 hours prior to cardiac arrest or ICU transfer versus 1.7 hours for standard Rapid Response Team activation.
Conclusions: Electronic Cardiac Arrest Risk Triage score identified significantly more cardiac arrests and ICU transfers than standard Rapid Response Team activation and did so many hours in advance.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Similar articles
-
Derivation of a cardiac arrest prediction model using ward vital signs*.Crit Care Med. 2012 Jul;40(7):2102-8. doi: 10.1097/CCM.0b013e318250aa5a. Crit Care Med. 2012. PMID: 22584764 Free PMC article.
-
Using electronic health record data to develop and validate a prediction model for adverse outcomes in the wards*.Crit Care Med. 2014 Apr;42(4):841-8. doi: 10.1097/CCM.0000000000000038. Crit Care Med. 2014. PMID: 24247472 Free PMC article.
-
Multicenter development and validation of a risk stratification tool for ward patients.Am J Respir Crit Care Med. 2014 Sep 15;190(6):649-55. doi: 10.1164/rccm.201406-1022OC. Am J Respir Crit Care Med. 2014. PMID: 25089847 Free PMC article.
-
Risk stratification of hospitalized patients on the wards.Chest. 2013 Jun;143(6):1758-1765. doi: 10.1378/chest.12-1605. Chest. 2013. PMID: 23732586 Free PMC article. Review.
-
Trigger Criteria: Big Data.Crit Care Clin. 2018 Apr;34(2):199-207. doi: 10.1016/j.ccc.2017.12.007. Epub 2018 Feb 1. Crit Care Clin. 2018. PMID: 29482900 Review.
Cited by
-
Advances in performance, more benefits... the perspectives of rapid response teams.Rev Bras Ter Intensiva. 2016 Sep;28(3):217-219. doi: 10.5935/0103-507X.20160048. Rev Bras Ter Intensiva. 2016. PMID: 27737425 Free PMC article. No abstract available.
-
Advancing In-Hospital Clinical Deterioration Prediction Models.Am J Crit Care. 2018 Sep;27(5):381-391. doi: 10.4037/ajcc2018957. Am J Crit Care. 2018. PMID: 30173171 Free PMC article.
-
Systematic review and longitudinal analysis of implementing Artificial Intelligence to predict clinical deterioration in adult hospitals: what is known and what remains uncertain.J Am Med Inform Assoc. 2024 Jan 18;31(2):509-524. doi: 10.1093/jamia/ocad220. J Am Med Inform Assoc. 2024. PMID: 37964688 Free PMC article.
-
Machine learning for dynamic and early prediction of acute kidney injury after cardiac surgery.J Thorac Cardiovasc Surg. 2023 Dec;166(6):e551-e564. doi: 10.1016/j.jtcvs.2022.09.045. Epub 2022 Oct 4. J Thorac Cardiovasc Surg. 2023. PMID: 36347651 Free PMC article.
-
Use of artificial intelligence in critical care: opportunities and obstacles.Crit Care. 2024 Apr 8;28(1):113. doi: 10.1186/s13054-024-04860-z. Crit Care. 2024. PMID: 38589940 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
