

Time-to-treatment of mental disorders in a community sample of Dutch adolescents. A TRAILS study
- PMID: 27075651
- PMCID: PMC6998684
- DOI: 10.1017/S2045796016000226
Time-to-treatment of mental disorders in a community sample of Dutch adolescents. A TRAILS study
Abstract
Aims: Timely recognition and treatment of mental disorders with an onset in childhood and adolescence is paramount, as these are characterized by greater severity and longer persistence than disorders with an onset in adulthood. Studies examining time-to-treatment, also referred to as treatment delay, duration of untreated illness or latency to treatment, and defined as the time between disorder onset and initial treatment contact, are sparse and all based on adult samples. The aim of this study was to describe time-to-treatment and its correlates for any health care professional (any care) and secondary mental health care (secondary care), for a broad range of mental disorders, in adolescents.
Methods: Data from the Dutch community-based cohort study TRacking Adolescents' Individual Lives Survey (TRAILS; N = 2230) were used. The Composite International Diagnostic Interview (CIDI) was administered to assess DSM-IV disorders, the age of onset, and the age of initial treatment contact with any health care professional in 1584 adolescents of 18-20 years old. In total 43% of the adolescents (n = 675) were diagnosed with a lifetime DSM-IV disorder. The age of initial treatment contact with secondary care was based on administrative records from 321 adolescents without a disorder onset before the age of 10. Descriptive statistics, cumulative lifetime probability plots, and Cox regression analyses were used analyze time-to-treatment.
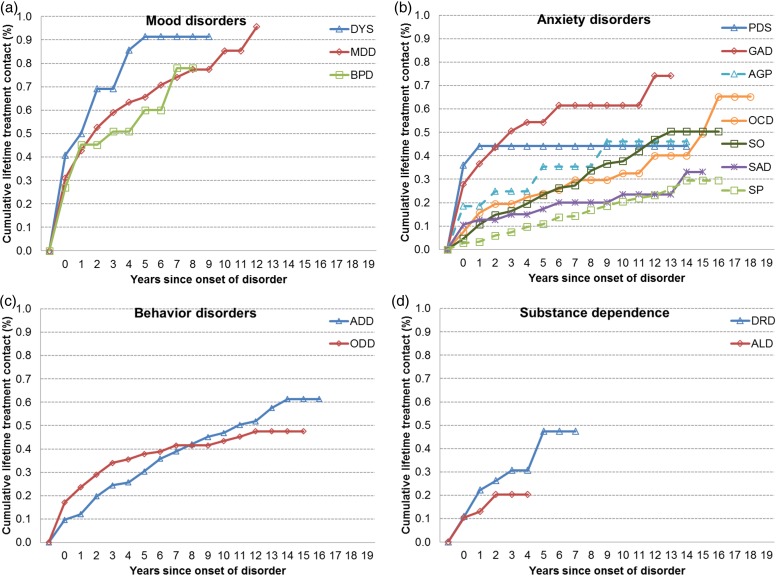
Results: The proportion of adolescents who reported lifetime treatment contact with any care varied from 15% for alcohol dependence to 82% for dysthymia. Regarding secondary care, proportions of lifetime treatment contact were lower for mood disorders and higher for substance dependence. Time-to-treatment for any care varied considerably between and within diagnostic classes. The probability of lifetime treatment contact for mood disorders was above 90%, whereas for other mental disorders this was substantially lower. An earlier age of onset predicted a longer, and the presence of a co-morbid mood disorder predicted a shorter time-to-treatment in general. Disorder severity predicted a shorter time-to-treatment for any care, but not for secondary care. Time-to-treatment for secondary care was shorter for adolescents from low and middle socioeconomic background than for adolescents from a high socioeconomic background.
Conclusion: Although the time-to-treatment was shorter for adolescents than for adults, it was still substantial, and the overall patterns were remarkably similar to those found in adults. Efforts to reduce time-to-treatment should therefore be aimed at children and adolescents. Future research should address mechanisms underlying time-to-treatment and its consequences for early-onset disorders in particular.
Keywords: Adolescence; diagnosis; health service research; mental health; survival analysis.
Figures
Similar articles
-
Delays in making initial treatment contact after the first onset of mental health disorders in the Argentinean Study of Mental Health Epidemiology.Epidemiol Psychiatr Sci. 2019 Apr;28(2):240-250. doi: 10.1017/S2045796018000094. Epub 2018 Mar 15. Epidemiol Psychiatr Sci. 2019. PMID: 29540248 Free PMC article.
-
Lifetime treatment contact and delay in treatment seeking after first onset of a mental disorder.Psychiatr Serv. 2013 Oct;64(10):981-9. doi: 10.1176/appi.ps.201200454. Psychiatr Serv. 2013. PMID: 23820725
-
Mental health in Dutch adolescents: a TRAILS report on prevalence, severity, age of onset, continuity and co-morbidity of DSM disorders.Psychol Med. 2015 Jan;45(2):345-60. doi: 10.1017/S0033291714001469. Epub 2014 Jun 20. Psychol Med. 2015. PMID: 25066533
-
[Mental health of children, adolescents and young adults--part 1: prevalence, illness persistence, adversities, service use, treatment delay and consequences].Fortschr Neurol Psychiatr. 2013 Nov;81(11):614-27. doi: 10.1055/s-0033-1355843. Epub 2013 Nov 5. Fortschr Neurol Psychiatr. 2013. PMID: 24194055 Review. German.
-
Age of onset of mental disorders and use of mental health services: needs, opportunities and obstacles.Epidemiol Psychiatr Sci. 2012 Mar;21(1):47-57. doi: 10.1017/s2045796011000746. Epidemiol Psychiatr Sci. 2012. PMID: 22670412 Review.
Cited by
-
A Smartphone Serious Game for Adolescents (Grow It! App): Development, Feasibility, and Acceptance Study.JMIR Form Res. 2022 Mar 3;6(3):e29832. doi: 10.2196/29832. JMIR Form Res. 2022. PMID: 35238795 Free PMC article.
-
Parent-perceived barriers to accessing services for their child's mental health problems.Child Adolesc Psychiatry Ment Health. 2021 Jan 29;15(1):4. doi: 10.1186/s13034-021-00357-7. Child Adolesc Psychiatry Ment Health. 2021. PMID: 33514400 Free PMC article.
-
Attitudes Toward and Familiarity With Virtual Reality Therapy Among Practicing Cognitive Behavior Therapists: A Cross-Sectional Survey Study in the Era of Consumer VR Platforms.Front Psychol. 2019 Feb 8;10:176. doi: 10.3389/fpsyg.2019.00176. eCollection 2019. Front Psychol. 2019. PMID: 30800086 Free PMC article.
-
Barriers to Access to Care Evaluation Scale - Proxy Report (BACE-PR): Evidence of Reliability and Validity for Caregivers Reporting on Children and Adolescents with Mental Health Concerns in Greece.Adm Policy Ment Health. 2025 Aug 25. doi: 10.1007/s10488-025-01466-7. Online ahead of print. Adm Policy Ment Health. 2025. PMID: 40850964
-
The predictive validity of the Strengths and Difficulties Questionnaire in preschool age to identify mental disorders in preadolescence.PLoS One. 2019 Jun 3;14(6):e0217707. doi: 10.1371/journal.pone.0217707. eCollection 2019. PLoS One. 2019. PMID: 31158249 Free PMC article.
References
-
- Achenbach TM, Rescorla LA (2001). Manual for the ASEBA School-Age Forms & Profiles. University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT.
-
- Altamura AC, Dell'Osso B, Mundo E, Dell'Osso L (2007). Duration of untreated illness in major depressive disorder: a naturalistic study. International Journal of Clinical Practice 61, 1697–1700. - PubMed
-
- Altamura AC, Dell'Osso B, Vismara S, Mundo E (2008). May duration of untreated illness influence the long-term course of major depressive disorder? European Psychiatry 23, 92–96. - PubMed
-
- Altamura AC, Buoli M, Albano A, Dell'Osso B (2010). Age at onset and latency to treatment (duration of untreated illness) in patients with mood and anxiety disorders: a naturalistic study. International Clinical Psychopharmacology 25, 172–179. - PubMed
-
- American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders, 4th edn APA: Washington, DC.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
