

Comfort and patient-centred care without excessive sedation: the eCASH concept
- PMID: 27075762
- PMCID: PMC4846689
- DOI: 10.1007/s00134-016-4297-4
Comfort and patient-centred care without excessive sedation: the eCASH concept
Abstract
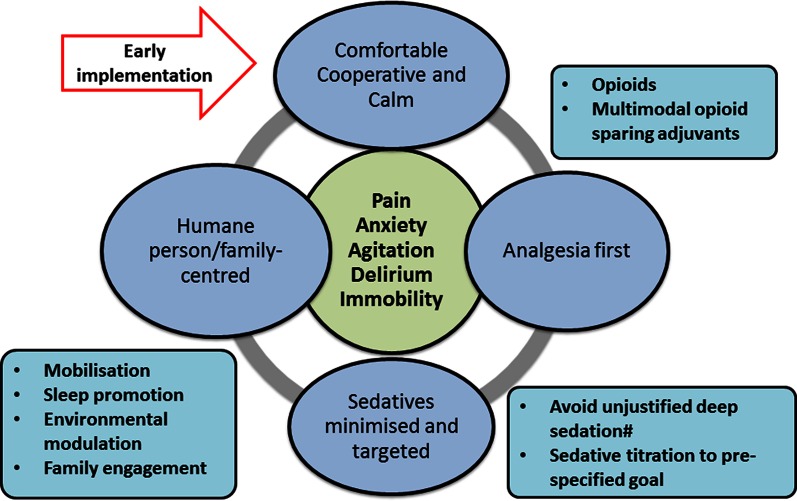
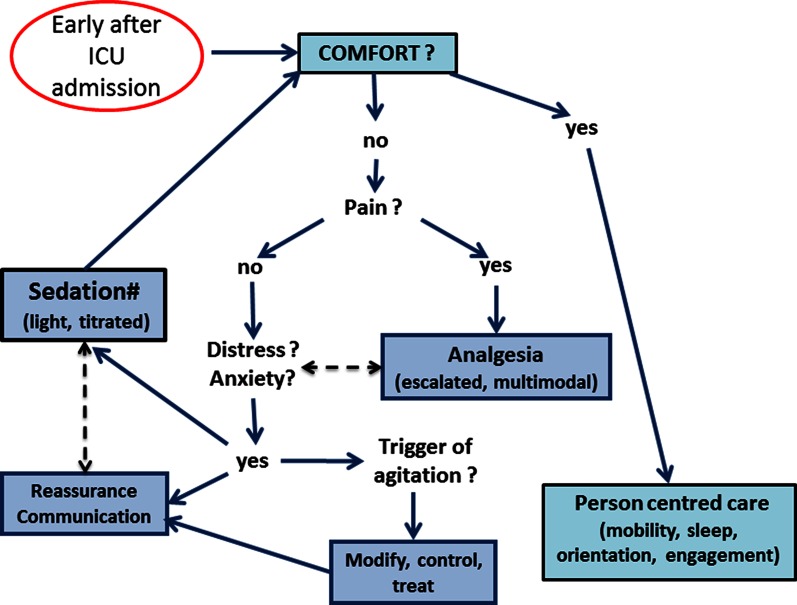
We propose an integrated and adaptable approach to improve patient care and clinical outcomes through analgesia and light sedation, initiated early during an episode of critical illness and as a priority of care. This strategy, which may be regarded as an evolution of the Pain, Agitation and Delirium guidelines, is conveyed in the mnemonic eCASH-early Comfort using Analgesia, minimal Sedatives and maximal Humane care. eCASH aims to establish optimal patient comfort with minimal sedation as the default presumption for intensive care unit (ICU) patients in the absence of recognised medical requirements for deeper sedation. Effective pain relief is the first priority for implementation of eCASH: we advocate flexible multimodal analgesia designed to minimise use of opioids. Sedation is secondary to pain relief and where possible should be based on agents that can be titrated to a prespecified target level that is subject to regular review and adjustment; routine use of benzodiazepines should be minimised. From the outset, the objective of sedation strategy is to eliminate the use of sedatives at the earliest medically justifiable opportunity. Effective analgesia and minimal sedation contribute to the larger aims of eCASH by facilitating promotion of sleep, early mobilization strategies and improved communication of patients with staff and relatives, all of which may be expected to assist rehabilitation and avoid isolation, confusion and possible long-term psychological complications of an ICU stay. eCASH represents a new paradigm for patient-centred care in the ICU. Some organizational challenges to the implementation of eCASH are identified.
Keywords: Analgesia; ICU; Pain; Sedation; eCASH.
Figures
Comment in
-
Monitoring pain-sedation-delirium in ICU: the Cinderella of analgo-sedation strategy?Minerva Anestesiol. 2017 Feb;83(2):131-133. doi: 10.23736/S0375-9393.17.11764-5. Minerva Anestesiol. 2017. PMID: 28190321 No abstract available.
References
-
- Shehabi Y, Chan L, Kadiman S, Alias A, Ismail WN, Tan MA, Khoo TM, Ali SB, Saman MA, Shaltut A, Tan CC, Yong CY, Bailey M. Sedation depth and long-term mortality in mechanically ventilated critically ill adults: a prospective longitudinal multicentre cohort study. Intensive Care Med. 2013;39:910–918. doi: 10.1007/s00134-013-2830-2. - DOI - PMC - PubMed
-
- Tanaka LM, Azevedo LC, Park M, Schettino G, Nassar AP, Réa-Neto A, Tannous L, de Souza-Dantas VC, Torelly A, Lisboa T, et al. Early sedation and clinical outcomes of mechanically ventilated patients: a prospective multicenter cohort study. Crit Care. 2014;18:R156. doi: 10.1186/cc13995. - DOI - PMC - PubMed
-
- Brummel NE, Jackson JC, Pandharipande PP, Thompson JL, Shintani AK, Dittus RS, Gill TM, Bernard GR, Ely EW, Girard TD. Delirium in the ICU and subsequent long-term disability among survivors of mechanical ventilation. Crit Care Med. 2014;42:369–377. doi: 10.1097/CCM.0b013e3182a645bd. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
