

Accuracy of delivered airway pressure and work of breathing estimation during proportional assist ventilation: a bench study
- PMID: 27076185
- PMCID: PMC4830790
- DOI: 10.1186/s13613-016-0131-y
Accuracy of delivered airway pressure and work of breathing estimation during proportional assist ventilation: a bench study
Abstract
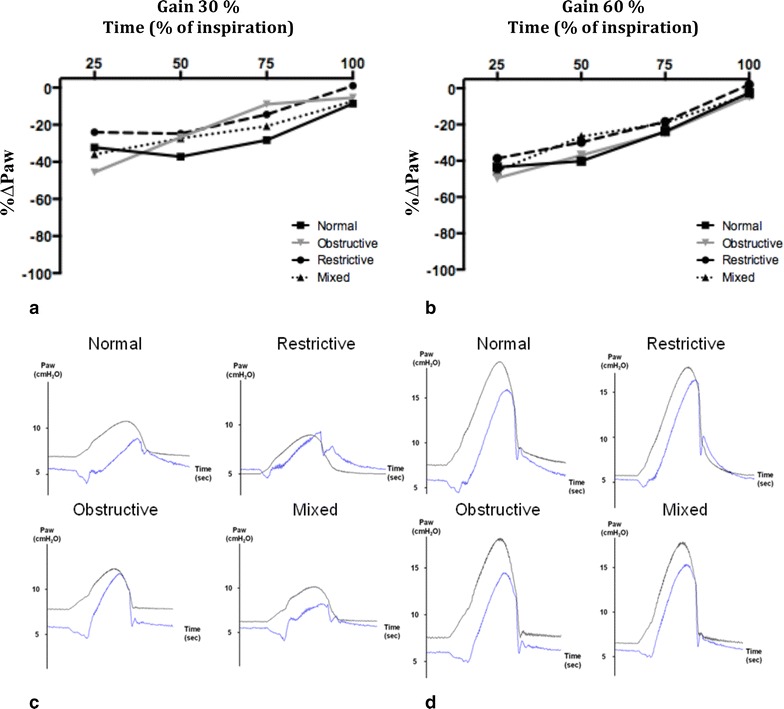
Background: Proportional assist ventilation+ (PAV+) delivers airway pressure (P aw) in proportion to patient effort (P mus) by using the equation of motion of the respiratory system. PAV+ calculates automatically respiratory mechanics (elastance and resistance); the work of breathing (WOB) is estimated by the ventilator. The accuracy of P mus estimation and hence accuracy of the delivered P aw and WOB calculation have not been assessed. This study aimed at assessing the accuracy of delivered P aw and calculated WOB by PAV+ and examining the factors influencing this accuracy.
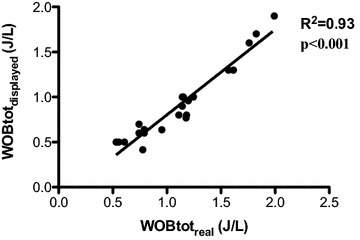
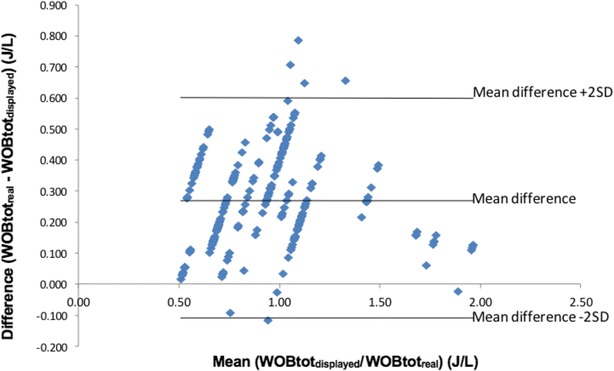
Methods: Using an active lung model with different respiratory mechanics, we compared (1) the actual delivered P aw by the ventilator to the theoretical P aw as defined by the equation of motion and (2) the WOB value displayed by the ventilator to the WOB measured from a Campbell diagram.
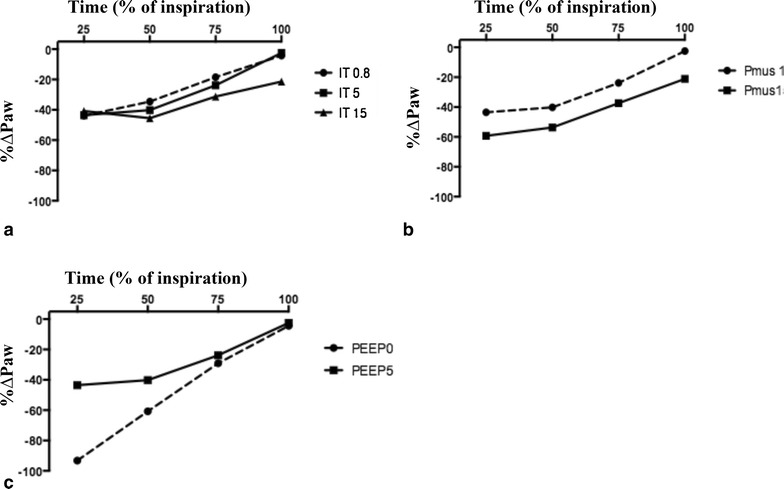
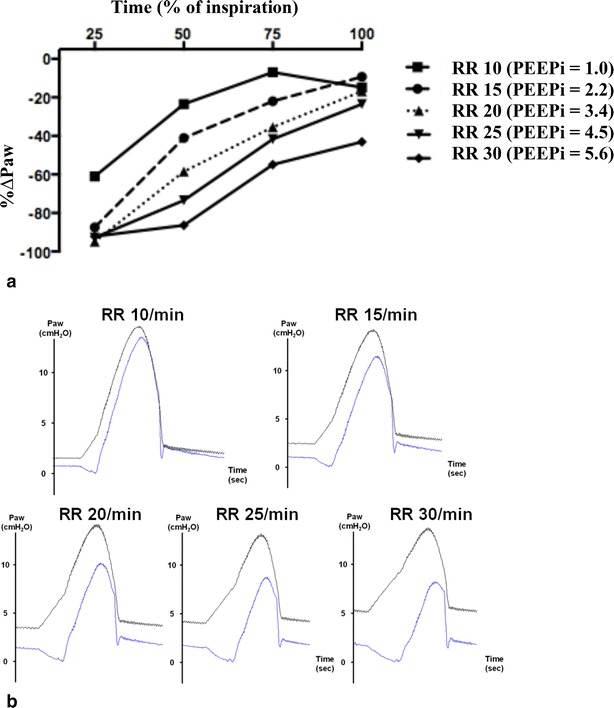
Results: Irrespective of respiratory mechanics and gain, the ventilator provided a P aw approximately 25 % lower than expected. This underassistance was greatest at the beginning of the inspiration. Intrinsic PEEP (PEEPi), associated with an increase in trigger delay, was a major factor affecting PAV+ accuracy. The absolute value of total WOB displayed by the ventilator was underestimated, but the changes in WOB were accurately detected by the ventilator.
Conclusion: The assistance provided by PAV+ well follows P mus but with a constant underassistance. This is associated with an underestimation by the ventilator of the WOB. PEEPi can be a major factor contributing to PAV+ inaccuracy. Clinical recommendations should include using a high trigger sensitivity and a careful PEEP titration.
Figures
References
-
- Delaere S, Roeseler J, D’hoore W, Matte P, Reynaert M, Jolliet P, Sottiaux T, Liistro G. Respiratory muscle workload in intubated, spontaneously breathing patients without COPD: pressure support vs proportional assist ventilation. Intensive Care Med. 2003;29:949–954. doi: 10.1007/s00134-003-1704-4. - DOI - PubMed
-
- Ranieri VM, Grasso S, Mascia L, Martino S, Fiore T, Brienza A, Giuliani R. Effects of proportional assist ventilation on inspiratory muscle effort in patients with chronic obstructive pulmonary disease and acute respiratory failure. Anesthesiology. 1997;86:79–91. doi: 10.1097/00000542-199701000-00012. - DOI - PubMed
-
- Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Respiratory load compensation during mechanical ventilation—proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med. 2006;32:692–699. doi: 10.1007/s00134-006-0110-0. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
