

Biomarker kinetics in the prediction of VAP diagnosis: results from the BioVAP study
- PMID: 27076187
- PMCID: PMC4830786
- DOI: 10.1186/s13613-016-0134-8
Biomarker kinetics in the prediction of VAP diagnosis: results from the BioVAP study
Abstract
Background: Prediction of diagnosis of ventilator-associated pneumonia (VAP) remains difficult. Our aim was to assess the value of biomarker kinetics in VAP prediction.
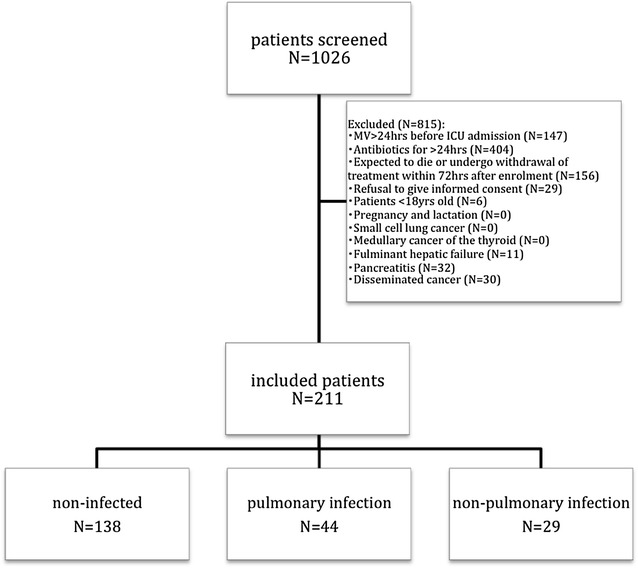
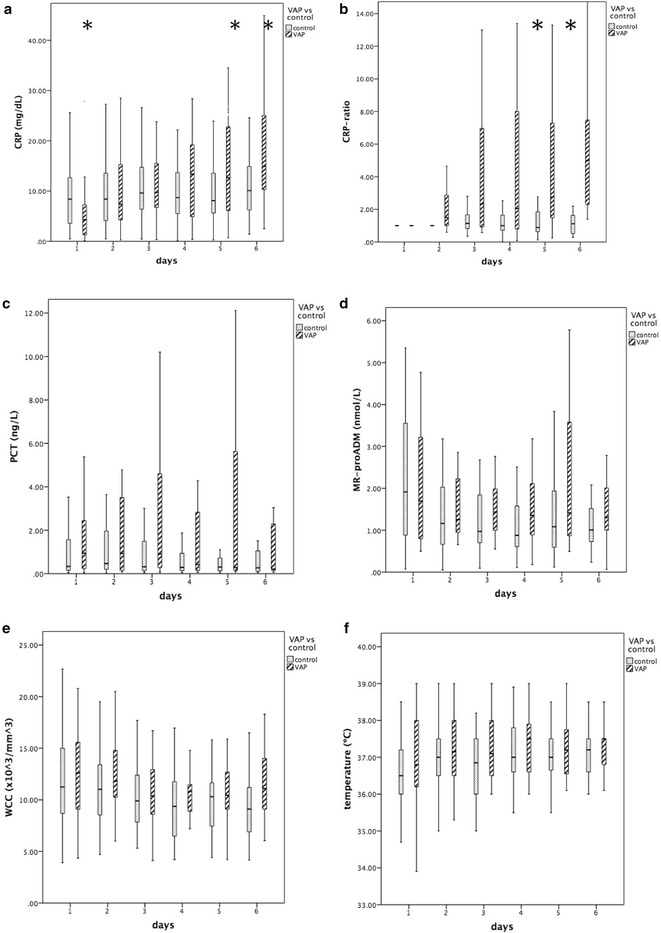
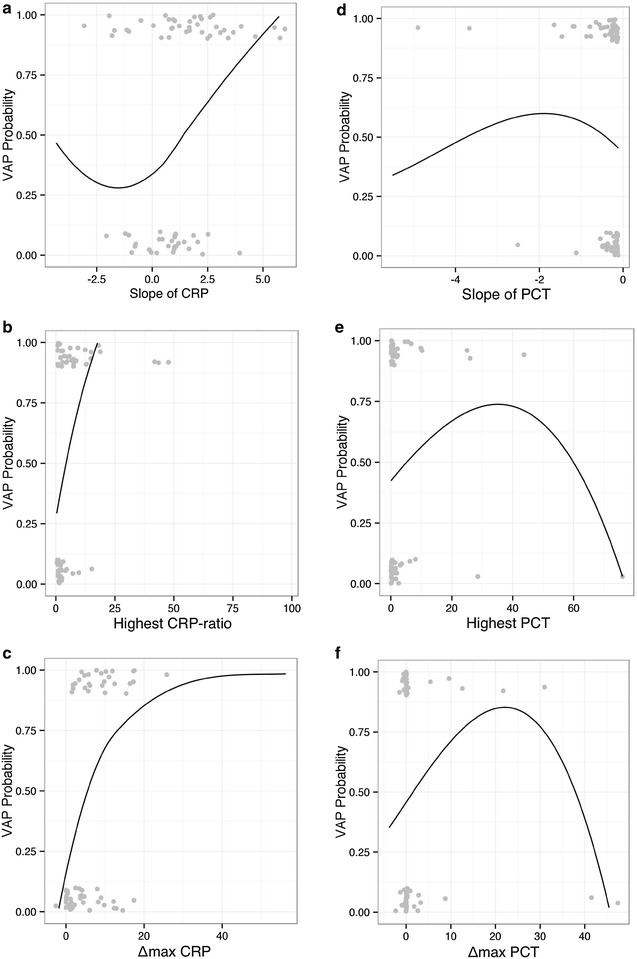
Methods: We performed a prospective, multicenter, observational study to evaluate predictive accuracy of biomarker kinetics, namely C-reactive protein (CRP), procalcitonin (PCT), mid-region fragment of pro-adrenomedullin (MR-proADM), for VAP management in 211 patients receiving mechanical ventilation for >72 h. For the present analysis, we assessed all (N = 138) mechanically ventilated patients without an infection at admission. The kinetics of each variable, from day 1 to day 6 of mechanical ventilation, was assessed with each variable's slopes (rate of biomarker change per day), highest level and maximum amplitude of variation (Δ (max)).
Results: A total of 35 patients (25.4 %) developed a VAP and were compared with 70 non-infected controls (50.7 %). We excluded 33 patients (23.9 %) who developed a non-VAP nosocomial infection. Among the studied biomarkers, CRP and CRP ratio showed the best performance in VAP prediction. The slope of CRP change over time (adjusted odds ratio [aOR] 1.624, confidence interval [CI]95% [1.206, 2.189], p = 0.001), the highest CRP ratio concentration (aOR 1.202, CI95% [1.061, 1.363], p = 0.004) and Δ (max) CRP (aOR 1.139, CI95% [1.039, 1.248], p = 0.006), during the first 6 days of mechanical ventilation, were all significantly associated with VAP development. Both PCT and MR-proADM showed a poor predictive performance as well as temperature and white cell count.
Conclusions: Our results suggest that in patients under mechanical ventilation, daily CRP monitoring was useful in VAP prediction. Trial registration NCT02078999.
Keywords: Biomarkers; C-reactive protein; Clinical Pulmonary Infection Score; Diagnosis; Mid-region fragment of pro-adrenomedullin; Prediction; Procalcitonin; Ventilator-associated pneumonia.
Figures
References
-
- Determann RM, Millo JL, Gibot S, Korevaar JC, Vroom MB, van der Poll T, et al. Serial changes in soluble triggering receptor expressed on myeloid cells in the lung during development of ventilator-associated pneumonia. Intensive Care Med. 2005;31(11):1495–1500. doi: 10.1007/s00134-005-2818-7. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
