

Biological and Epidemiological Features of Antibiotic-Resistant Streptococcus pneumoniae in Pre- and Post-Conjugate Vaccine Eras: a United States Perspective
- PMID: 27076637
- PMCID: PMC4861989
- DOI: 10.1128/CMR.00058-15
Biological and Epidemiological Features of Antibiotic-Resistant Streptococcus pneumoniae in Pre- and Post-Conjugate Vaccine Eras: a United States Perspective
Abstract
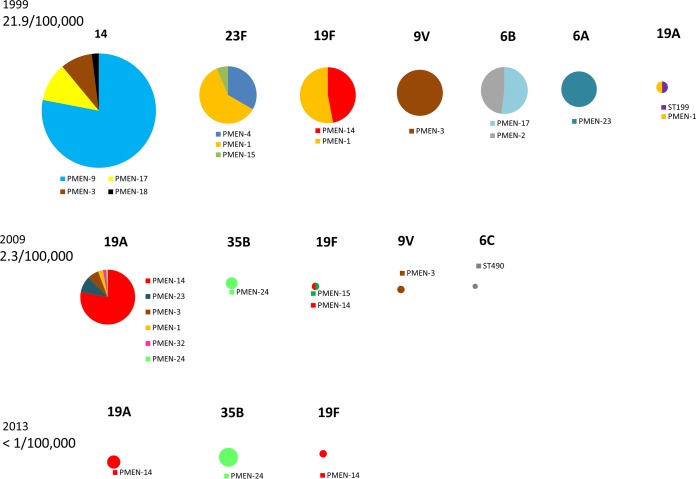
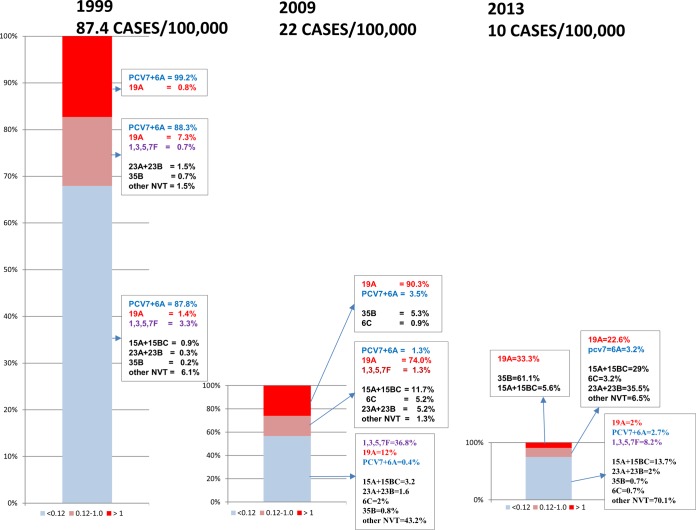
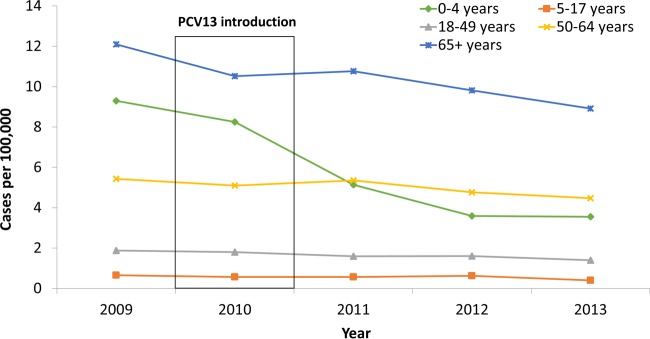
Streptococcus pneumoniae inflicts a huge disease burden as the leading cause of community-acquired pneumonia and meningitis. Soon after mainstream antibiotic usage, multiresistant pneumococcal clones emerged and disseminated worldwide. Resistant clones are generated through adaptation to antibiotic pressures imposed while naturally residing within the human upper respiratory tract. Here, a huge array of related commensal streptococcal strains transfers core genomic and accessory resistance determinants to the highly transformable pneumococcus. β-Lactam resistance is the hallmark of pneumococcal adaptability, requiring multiple independent recombination events that are traceable to nonpneumococcal origins and stably perpetuated in multiresistant clonal complexes. Pneumococcal strains with elevated MICs of β-lactams are most often resistant to additional antibiotics. Basic underlying mechanisms of most pneumococcal resistances have been identified, although new insights that increase our understanding are continually provided. Although all pneumococcal infections can be successfully treated with antibiotics, the available choices are limited for some strains. Invasive pneumococcal disease data compiled during 1998 to 2013 through the population-based Active Bacterial Core surveillance program (U.S. population base of 30,600,000) demonstrate that targeting prevalent capsular serotypes with conjugate vaccines (7-valent and 13-valent vaccines implemented in 2000 and 2010, respectively) is extremely effective in reducing resistant infections. Nonetheless, resistant non-vaccine-serotype clones continue to emerge and expand.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures




References
-
- Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, Jha P, Campbell H, Walker CF, Cibulskis R, Eisele T, Liu L, Mathers C, Child Health Epidemiology Reference Group of WHO and UNICEF. 2010. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet 375:1969–1987. doi: 10.1016/S0140-6736(10)60549-1. - DOI - PubMed
-
- World Health Organization. 2014. Global immunization data. World Health Organization, Geneva, Switzerland: http://www.who.int/immunization/monitoring_surveillance/global_immunizat... Accessed 17 September 2014.
-
- Centers for Disease Control and Prevention. 1993. Recommendations of the Advisory Committee on Immunization Practices (ACIP): use of vaccines and immunoglobulins in persons with altered immunocompetence. MMWR Morb Mortal Wkly Rep 42:1–18.
-
- Centers for Disease Control and Prevention. 1997. Prevention of pneumococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 46:1–24.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
