

Impact of clinical pharmacist in an Indian Intensive Care Unit
- PMID: 27076707
- PMCID: PMC4810937
- DOI: 10.4103/0972-5229.175931
Impact of clinical pharmacist in an Indian Intensive Care Unit
Abstract
Background and objectives: A critically ill patient is treated and reviewed by physicians from different specialties; hence, polypharmacy is a very common. This study was conducted to assess the impact and effectiveness of having a clinical pharmacist in an Indian Intensive Care Unit (ICU). It also evaluates the clinical pharmacist interventions with a focus on optimizing the quality of pharmacotherapy and patient safety.
Materials and methods: The prospective, observational study was carried out in medical and surgical/trauma ICU over a period of 1 year. All detected drug-related problems and interventions were categorized based on the Pharmaceutical Care Network Europe system.
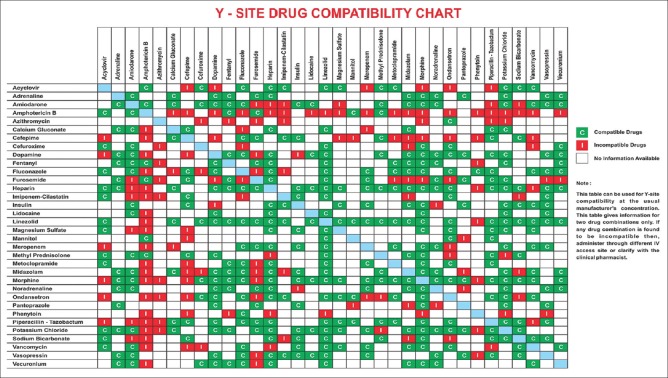
Results: During the study period, average monthly census of 1032 patients got treated in the ICUs. A total of 986 pharmaceutical interventions due to drug-related problems were documented, whereof medication errors accounted for 42.6% (n = 420), drug of choice problem 15.4% (n = 152), drug-drug interactions were 15.1% (n = 149), Y-site drug incompatibility was 13.7% (n = 135), drug dosing problems were 4.8% (n = 47), drug duplications reported were 4.6% (n = 45), and adverse drug reactions documented were 3.8% (n = 38). Drug dosing adjustment done by the clinical pharmacist included 140 (11.9%) renal dose, 62 (5.2%) hepatic dose, 17 (1.4%) pediatric dose, and 104 (8.8%) insulin dosing modifications. A total of 577 drug and poison information queries were answered by the clinical pharmacist.
Conclusion: Clinical pharmacist as a part of multidisciplinary team in our study was associated with a substantially lower rate of adverse drug event caused by medication errors, drug interactions, and drug incompatibilities.
Keywords: Adverse drug reaction; critical care pharmacist; drug interaction; medication error.
Figures

References
-
- Kane-Gill SL, Jacobi J, Rothschild JM. Adverse drug events in intensive care units: Risk factors, impact, and the role of team care. Crit Care Med. 2010;38(6 Suppl):S83–9. - PubMed
-
- Haupt MT, Bekes CE, Brilli RJ, Carl LC, Gray AW, Jastremski MS, et al. Guidelines on critical care services and personnel: Recommendations based on a system of categorization of three levels of care. Crit Care Med. 2003;31:2677–83. - PubMed
-
- Rudis MI, Brandl KM. Position paper on critical care pharmacy services. Society of Critical Care Medicine and American College of Clinical Pharmacy Task Force on Critical Care Pharmacy Services. Crit Care Med. 2000;28:3746–50. - PubMed
-
- Boyko WL, Jr, Yurkowski PJ, Ivey MF, Armitstead JA, Roberts BL. Pharmacist influence on economic and morbidity outcomes in a tertiary care teaching hospital. Am J Health Syst Pharm. 1997;54:1591–5. - PubMed
-
- Smythe MA, Shah PP, Spiteri TL, Lucarotti RL, Begle RL. Pharmaceutical care in medical progressive care patients. Ann Pharmacother. 1998;32:294–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources