

Risk factors for local recurrence after en bloc endoscopic submucosal dissection for early gastric cancer
- PMID: 27076871
- PMCID: PMC4823671
- DOI: 10.4253/wjge.v8.i7.330
Risk factors for local recurrence after en bloc endoscopic submucosal dissection for early gastric cancer
Abstract
Aim: To investigate factors related to recurrence following en bloc resection using endoscopic submucosal dissection (ESD) in patients with early gastric cancer (EGC).
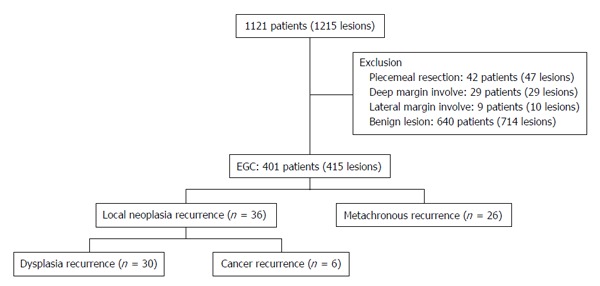
Methods: A total of 1121 patients (1215 lesions) who had undergone ESD for gastric neoplasia between April 2003 and May 2010 were retrospectively reviewed. Data from 401 patients (415 lesions) were analyzed, following the exclusion of those who underwent piecemeal resection, with deep resection margin invasion or lateral margin infiltration, and diagnosed with benign lesions.
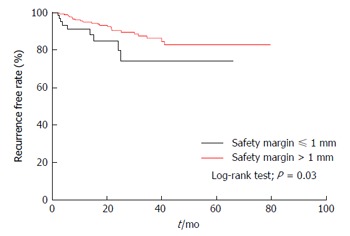
Results: Local recurrence after en bloc ESD was found in 36 cases (8.7%). Unclear resection margins, long procedure times, and narrow safety margins were identified as risk factors for recurrence. Lesions located in the upper third of the stomach showed a higher rate of recurrence than those located in the lower third of the stomach (OR = 2.9, P = 0.03). The probability of no recurrence for up to 24 mo was 79.9% in those with a safety resection margin ≤ 1 mm and 89.5% in those with a margin > 1 mm (log-rank test, P = 0.03).
Conclusion: Even in cases in which en bloc ESD is performed for EGC, local recurrence still occurs. To reduce local recurrences, more careful assessment will be needed prior to the implementation of ESD in cases in which the tumor is located in the upper third of the stomach. In addition, clear identification of tumor boundaries as well as the securing of sufficient safety resection margins will be important.
Keywords: Early gastric cancer; En bloc resection; Endoscopic mucosal resection; Endoscopic submucosal dissection; Recurrence.
Figures
Similar articles
-
AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States.Clin Gastroenterol Hepatol. 2019 Jan;17(1):16-25.e1. doi: 10.1016/j.cgh.2018.07.041. Epub 2018 Aug 2. Clin Gastroenterol Hepatol. 2019. PMID: 30077787 Review.
-
Recurrence rate of lateral margin-positive cases after en bloc endoscopic submucosal dissection of colorectal neoplasia.Int J Colorectal Dis. 2018 Jun;33(6):735-743. doi: 10.1007/s00384-018-3012-z. Epub 2018 Mar 12. Int J Colorectal Dis. 2018. PMID: 29532207
-
Endoscopic submucosal dissection for early gastric cancer: a large-scale feasibility study.Gut. 2009 Mar;58(3):331-6. doi: 10.1136/gut.2008.165381. Epub 2008 Nov 10. Gut. 2009. PMID: 19001058
-
[Efficacy comparison between surgical resection and endoscopic submucosal dissection of early gastric cancer in a domestic single center].Zhonghua Wei Chang Wai Ke Za Zhi. 2018 Feb 25;21(2):190-195. Zhonghua Wei Chang Wai Ke Za Zhi. 2018. PMID: 29492919 Chinese.
-
Endoscopic Submucosal Dissection of Early Gastric Cancer with Mixed-Type Histology: A Systematic Review.Dig Dis Sci. 2020 Jan;65(1):276-291. doi: 10.1007/s10620-019-05761-w. Epub 2019 Jul 31. Dig Dis Sci. 2020. PMID: 31367880
Cited by
-
Clinical outcome of non-curative endoscopic submucosal dissection for early gastric cancer.J Gastrointest Oncol. 2024 Apr 30;15(2):566-576. doi: 10.21037/jgo-24-168. Epub 2024 Apr 28. J Gastrointest Oncol. 2024. PMID: 38756642 Free PMC article.
-
Endoscopic Submucosal Tunnel Dissection for Large Gastric Neoplastic Lesions: A Case-Matched Controlled Study.Gastroenterol Res Pract. 2018 Mar 6;2018:1419369. doi: 10.1155/2018/1419369. eCollection 2018. Gastroenterol Res Pract. 2018. PMID: 29692806 Free PMC article.
-
Early gastric cancer recurrence after endoscopic submucosal dissection: Not to be ignored!World J Gastrointest Oncol. 2024 Jan 15;16(1):8-12. doi: 10.4251/wjgo.v16.i1.8. World J Gastrointest Oncol. 2024. PMID: 38292847 Free PMC article.
-
Expression of macrophage inhibitory cytokine-1 in early gastric cancer cases treated using endoscopic mucosal resection and the correlation with prognosis.Oncol Lett. 2017 Aug;14(2):1967-1970. doi: 10.3892/ol.2017.6376. Epub 2017 Jun 13. Oncol Lett. 2017. PMID: 28789430 Free PMC article.
-
Prognostic factors for ESD of early gastric cancers: a systematic review and meta-analysis.Endosc Int Open. 2020 Sep;8(9):E1144-E1155. doi: 10.1055/a-1201-3089. Epub 2020 Aug 31. Endosc Int Open. 2020. PMID: 32904802 Free PMC article. Review.
References
-
- Kim SG. Endoscopic Resection of Early Gastric Cancer. Korean J Gastroenterol. 2009;54:77. - PubMed
-
- Nam SY, Choi IJ, Park KW, Kim CG, Lee JY, Kook MC, Lee JS, Park SR, Lee JH, Ryu KW, et al. Effect of repeated endoscopic screening on the incidence and treatment of gastric cancer in health screenees. Eur J Gastroenterol Hepatol. 2009;21:855–860. - PubMed
-
- Choi KD. Endoscopic resection of early gastric cancer. Korean J Med. 2011;81:40–46.
-
- Ono H. Endoscopic submucosal dissection for early gastric cancer. Chin J Dig Dis. 2005;6:119–121. - PubMed
-
- Oka S, Tanaka S, Kaneko I, Mouri R, Hirata M, Kawamura T, Yoshihara M, Chayama K. Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc. 2006;64:877–883. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
