

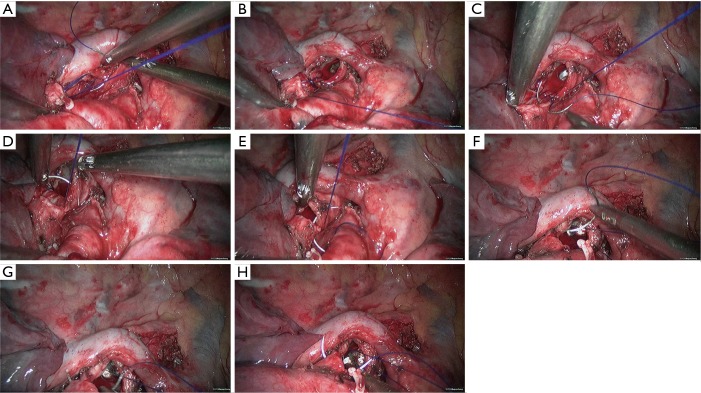
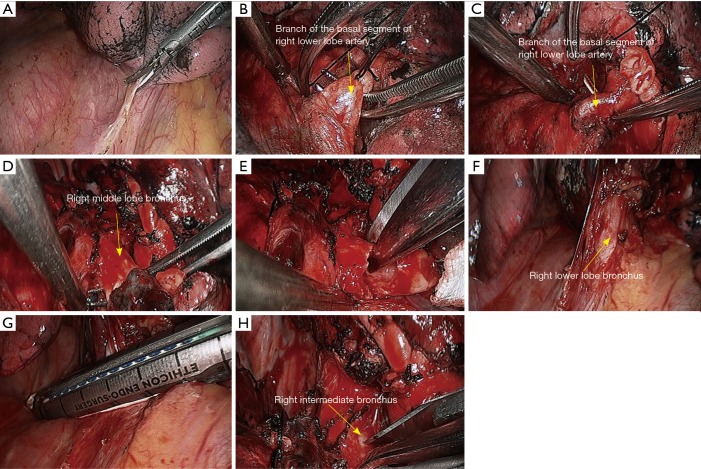
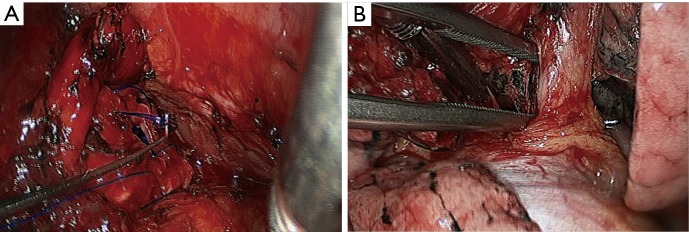
Complete video-assisted thoracoscopic surgery (VATS) bronchial sleeve lobectomy
- PMID: 27076954
- PMCID: PMC4805843
- DOI: 10.21037/jtd.2016.01.63
Complete video-assisted thoracoscopic surgery (VATS) bronchial sleeve lobectomy
Abstract
Background: To explore the effectiveness of video-assisted thoracoscopic surgery (VATS) bronchial sleeve resection and reconstruction.
Methods: The clinical data of patients who had received VATS bronchial sleeve lobectomy in our center from January 2008 to February 2015 were retrospectively analyzed.
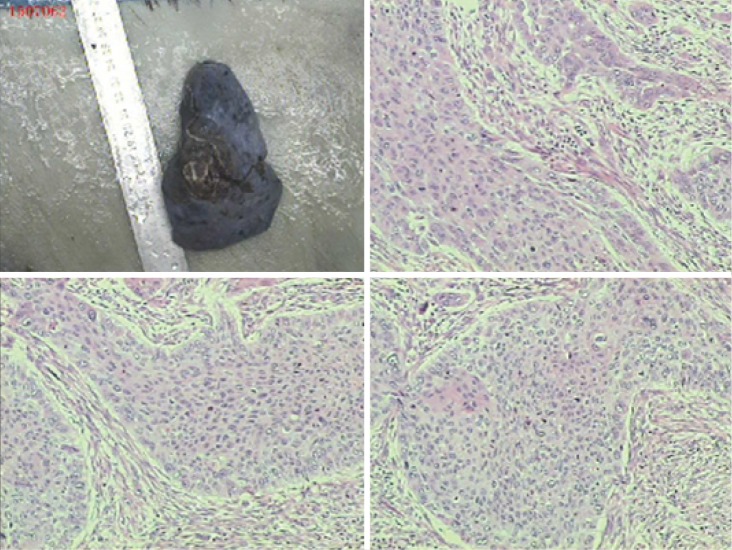
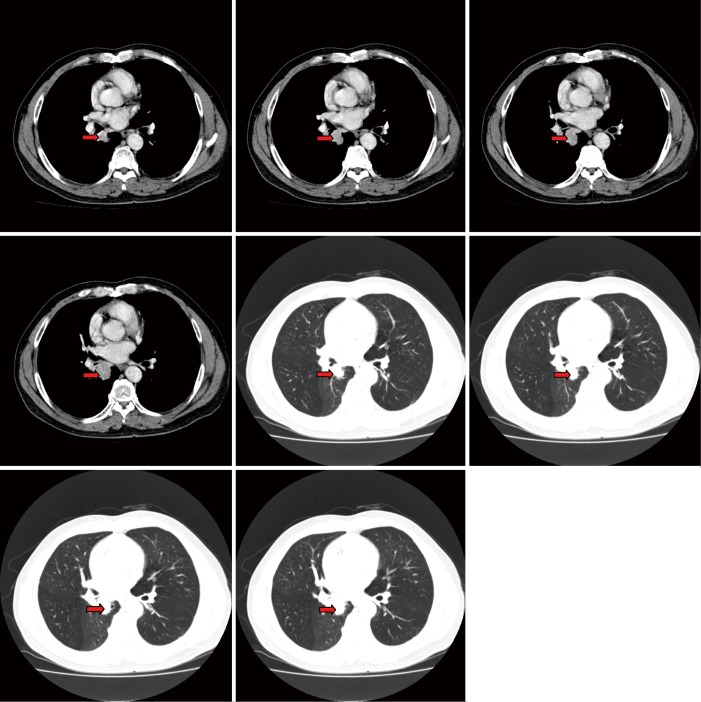
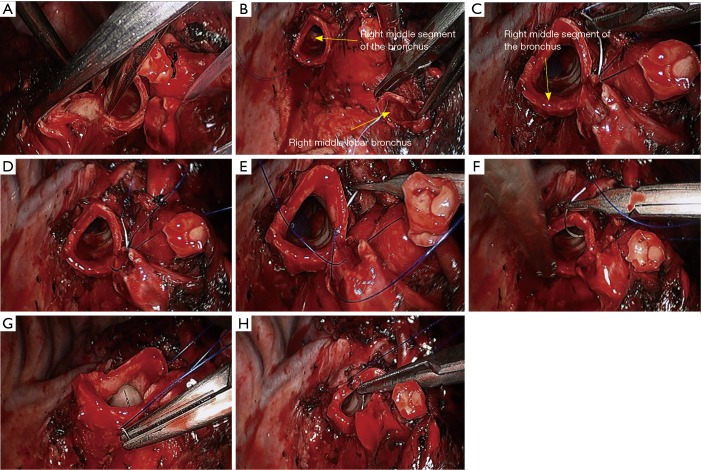
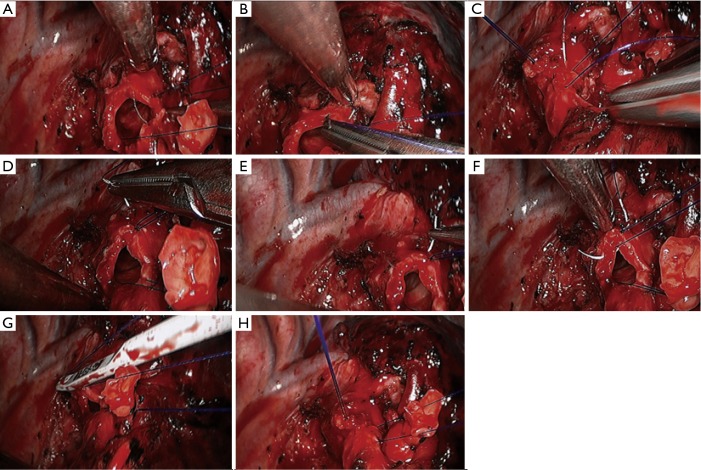
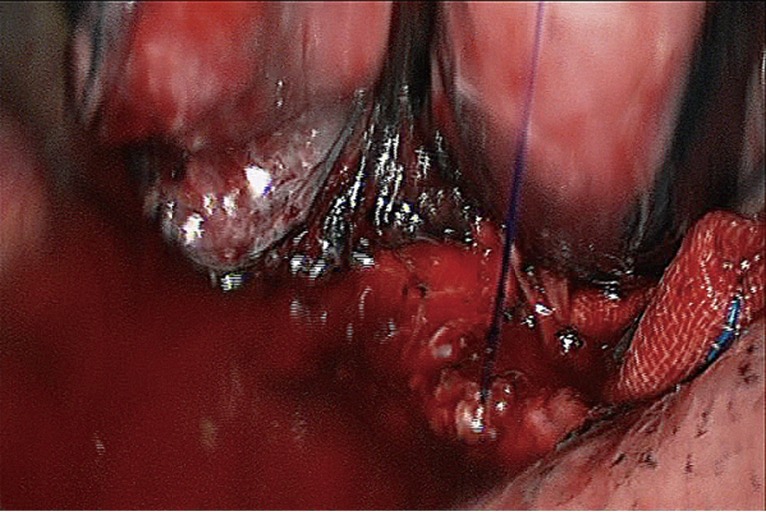
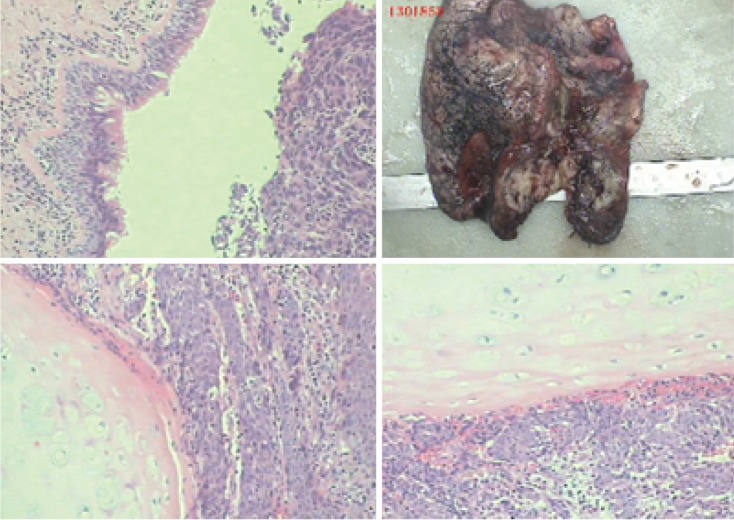
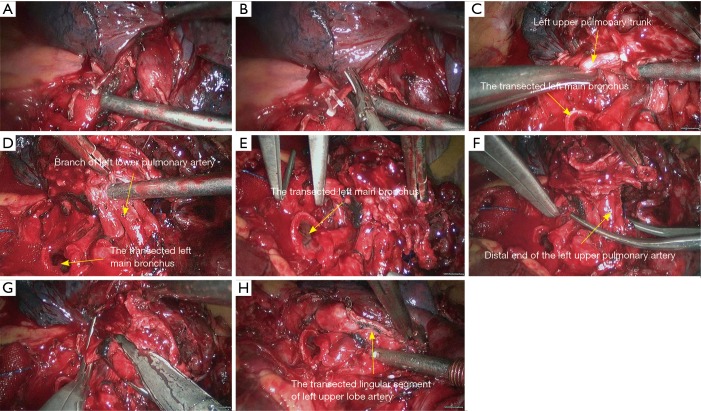
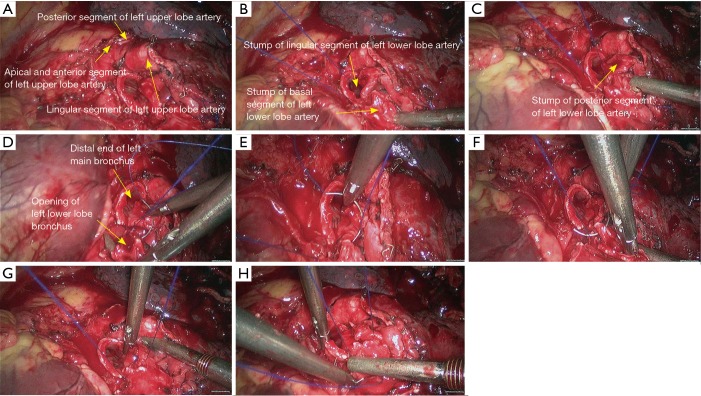
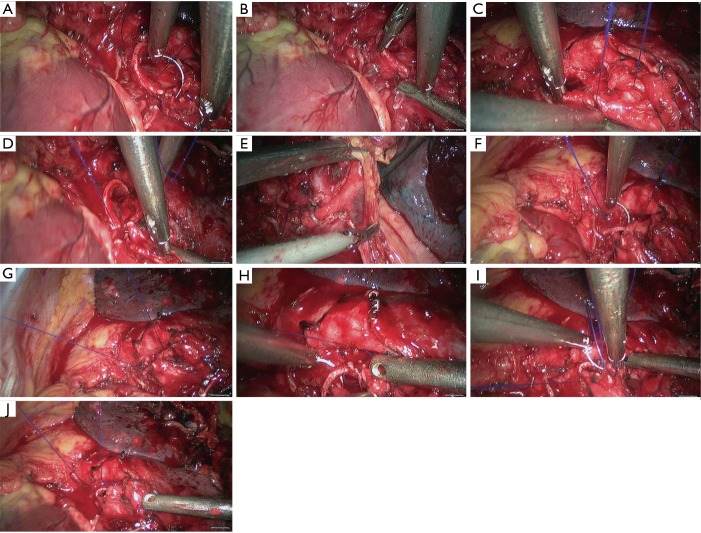
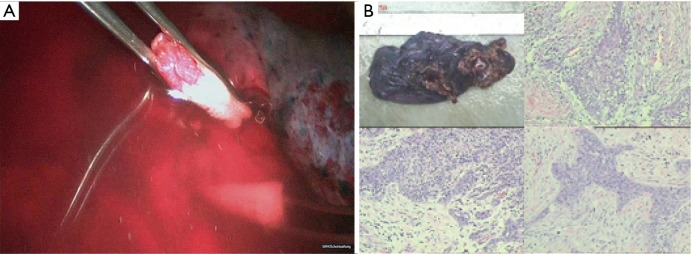
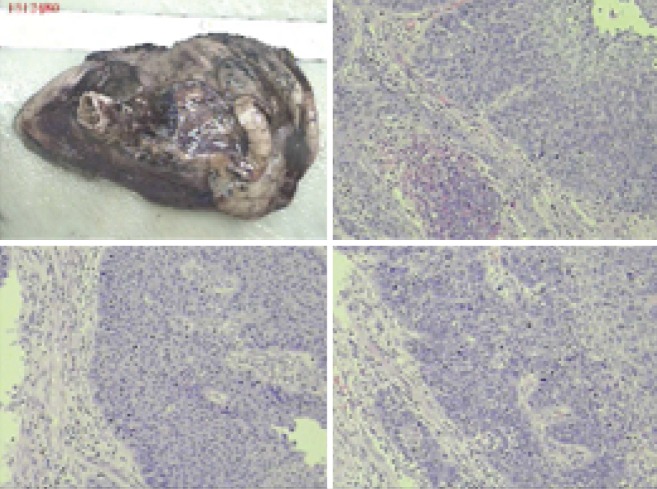
Results: Totally 118 patients (105 men and 13 women) received the VATS bronchial sleeve lobectomy. The procedures included sleeve resection of right upper lobe (n=59), right middle lobe (n=7), right lower lobe (n=8), left upper lobe (n=34), and left lower lobe (n=10). The lesions were confirmed to be squamous cell carcinoma (n=68), adenocarcinoma (n=16), mucoepidermoid carcinoma (n=8), adenosquamous carcinoma (n=7), large cell carcinoma (n=1), carcinoids (n=5), and others (n=13; including small cell carcinoma, pleomorphic carcinoma, and inflammatory myofibroblastic tumor). Operations lasted 118-223 min [mean ± standard deviations (SD): 124.00±31.75 min]. The length of removed bronchus was 1.50-2.00 cm (mean ± SD: 1.75±0.26 cm). The duration of bronchial anastomosis (from the first puncture to the completion of knotting) was 15-42 min (mean ± SD: 30.20±7.97 min). The number of dissected lymph node stations (at least three mediastinal lymph node stations, including station 7) was 5-9 stations (mean ± SD: 6.50±1.18 min). The number of dissected lymph nodes was 10-46 (mean ± SD: 26.00±10.48). The intraoperative blood loss was 20-400 mL (mean ± SD: 71.00±43.95 mL), and no blood transfusion was performed. All patients were observed in intensive care unit (ICU) for 1 day. Postoperative drainage was performed for 3-8 days (mean ± SD: 5.00±1.49 days). Postoperative hospital stay was 3-8 days (mean ± SD: 5.10±2.07 days).
Conclusions: VATS bronchial sleeve resection and reconstruction is a safe and feasible technique.
Keywords: Video-assisted thoracoscopic surgery (VATS); lobectomy; lung cancer; sleeve resection; surgery.
Conflict of interest statement
Figures






References
LinkOut - more resources
Full Text Sources
Other Literature Sources