

Non-intubated combined with video-assisted thoracoscopic in carinal reconstruction
- PMID: 27076956
- PMCID: PMC4805827
- DOI: 10.21037/jtd.2016.01.58
Non-intubated combined with video-assisted thoracoscopic in carinal reconstruction
Erratum in
-
Erratum to non-intubated combined with video-assisted thoracoscopic in carinal reconstruction.J Thorac Dis. 2016 Jul;8(7):E641. doi: 10.21037/jtd.2016.05.83. J Thorac Dis. 2016. PMID: 27499998 Free PMC article.
Abstract
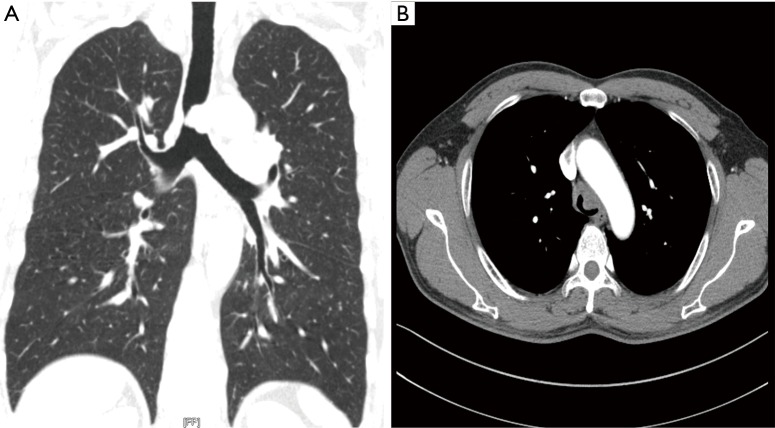
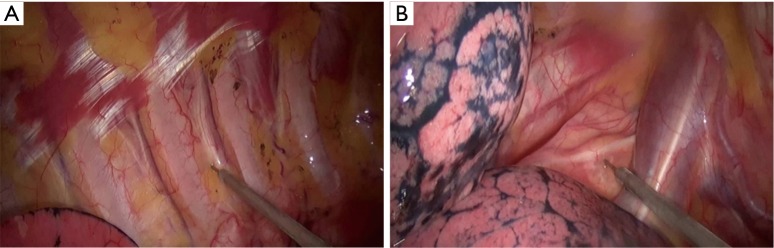
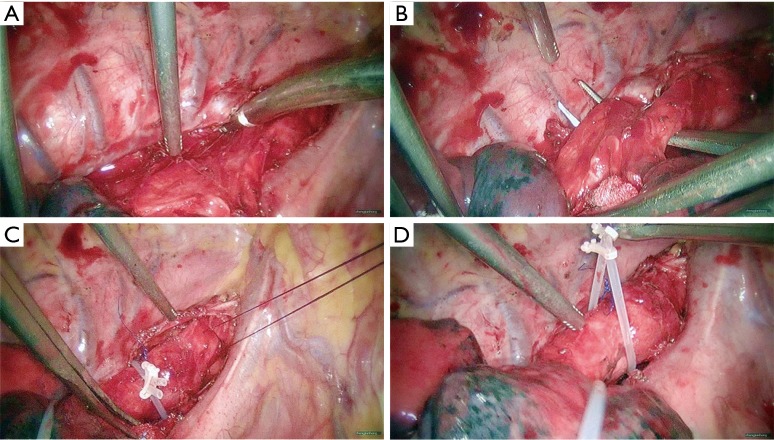
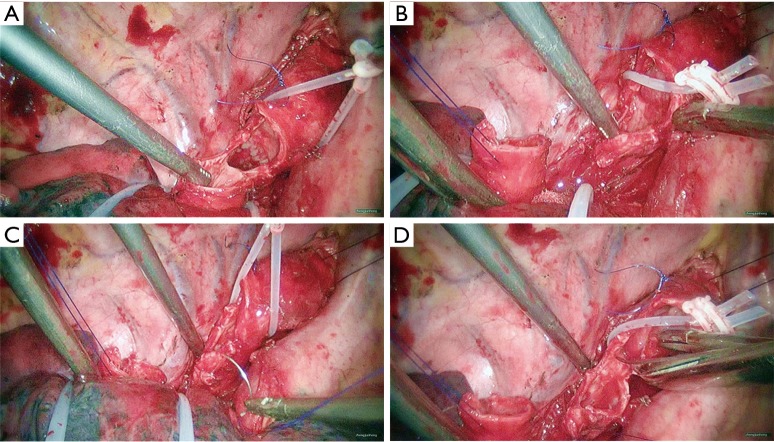
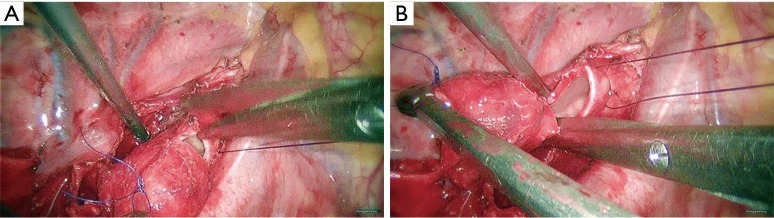
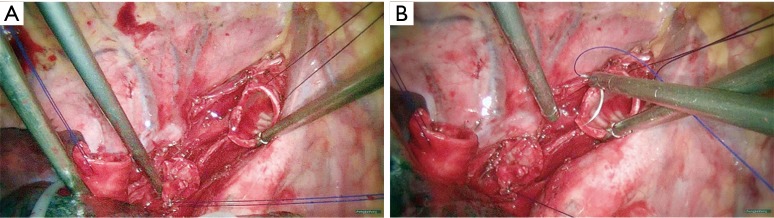
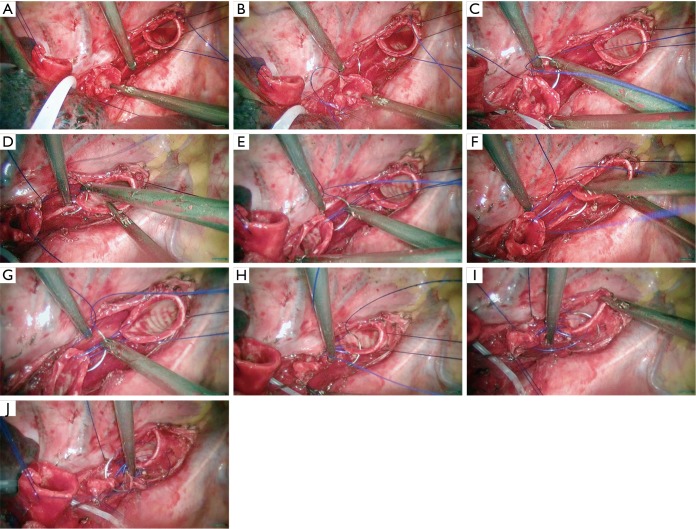
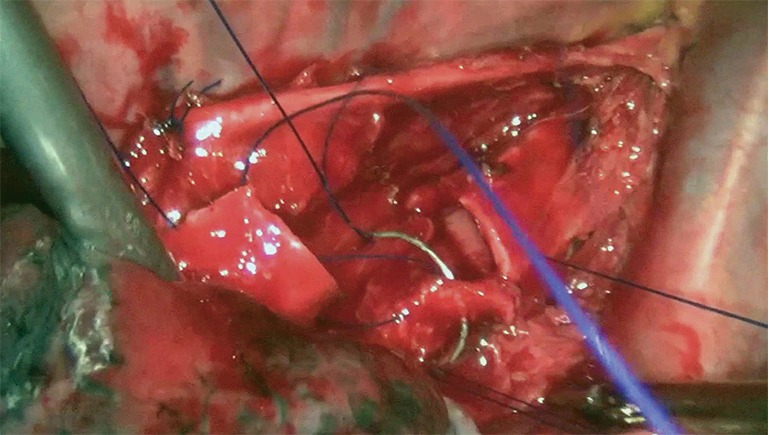
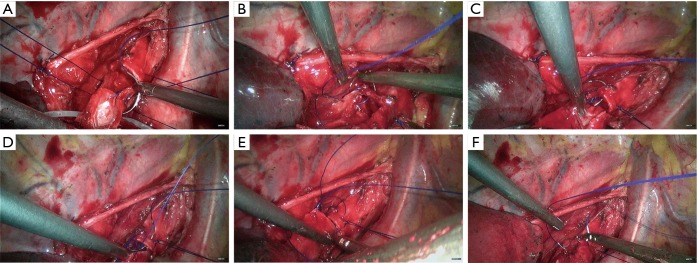
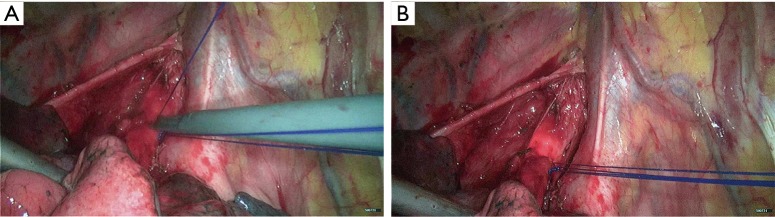
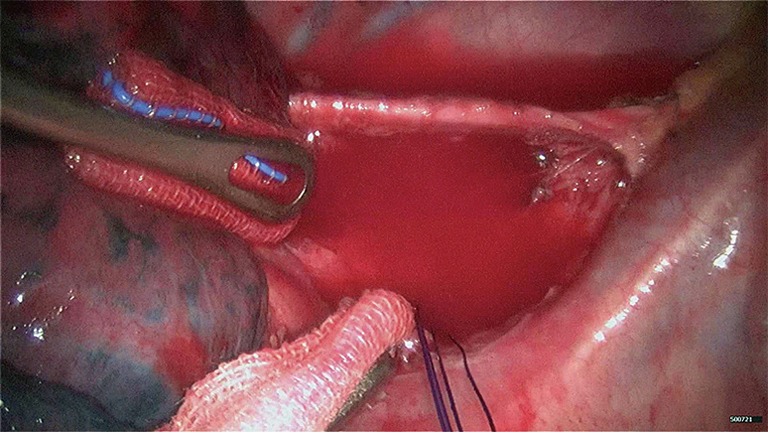
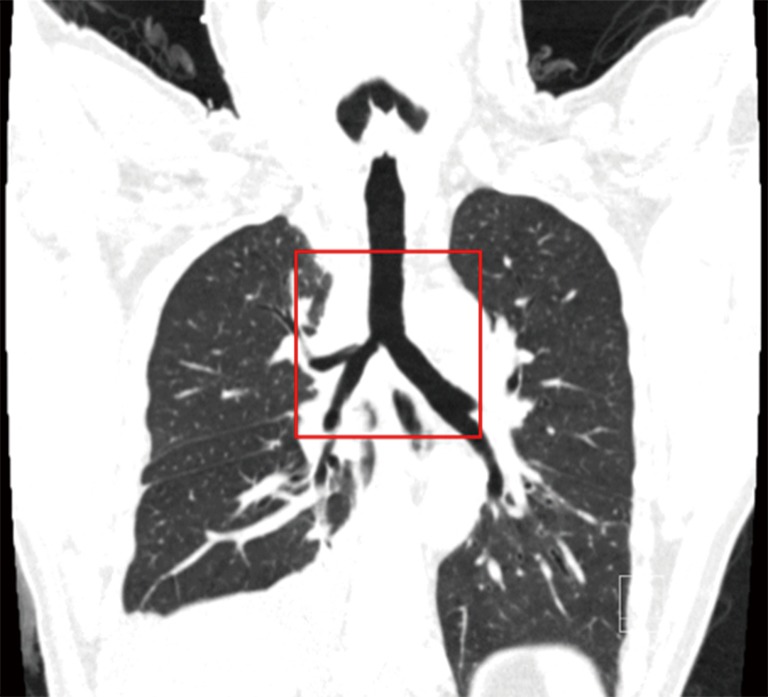
Carinal reconstruction is a difficult technique combined with video-assisted thoracoscopic surgery (VATS). It has a high requirement on the operator's skills in operating thoracoscope and meanwhile requires the close cooperation from anesthesiologists. Tracheal intubation and ventilator-assisted ventilation are key steps to ensure the success of surgery. However, tracheal intubation itself may influence the exposure of surgical field and increase the difficulty of anastomosis. In close cooperation of anesthesiologists, we did not perform tracheal intubation; rather, we carried out non-intubated complete VATS carinal reconstruction in a patient with adenoid cystic carcinoma (ACC) of the lower trachea. The awake complete VATS carinal reconstruction was successfully performed. The anastomosis lasted about 36 hours, and the whole surgical procedure lasted 230 min. The intraoperative blood loss was about 80 mL. The patient recovered well 100 min after surgery. A semi-solid diet began 6 hours following the surgery. This non-intubated anesthesia method makes the surgery easier, especially during the anastomosis of stumps. It is feasible and safe to apply this anesthesia technique in carinal reconstruction.
Keywords: Tracheal mass; awake; carinal reconstruction; video-assisted thoracoscopic surgery (VATS).
Conflict of interest statement
Figures


Comment in
-
Awake minimal invasive carinal resection-tightrope walking in thoracic surgery?J Thorac Dis. 2017 Oct;9(10):3667-3669. doi: 10.21037/jtd.2017.09.31. J Thorac Dis. 2017. PMID: 29268370 Free PMC article. No abstract available.
References
-
- Peng G, Cui F, He J, et al. Non-intubated combined with video-assisted thoracoscopic in carinal reconstruction. Asvide 2016;3:156. Available online: http://www.asvide.com/articles/911 - PMC - PubMed
-
- Mathey J, Binet JP, Galey JJ, et al. Tracheal and tracheobronchial resections; technique and results in 20 cases. J Thorac Cardiovasc Surg 1966;51:1-13. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical