

Video-assisted thoracoscopic surgery resection and reconstruction of thoracic trachea in the management of a tracheal neoplasm
- PMID: 27076958
- PMCID: PMC4805830
- DOI: 10.21037/jtd.2016.01.60
Video-assisted thoracoscopic surgery resection and reconstruction of thoracic trachea in the management of a tracheal neoplasm
Abstract
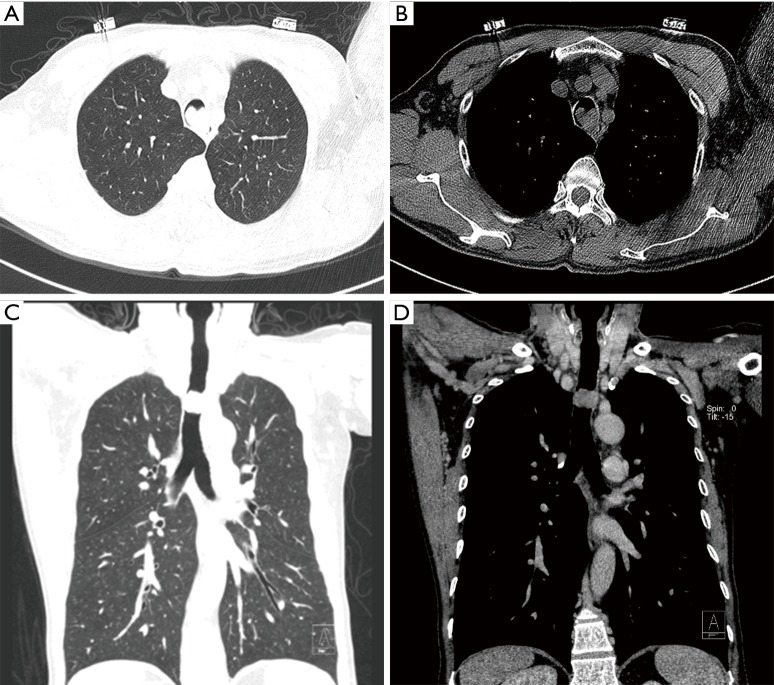
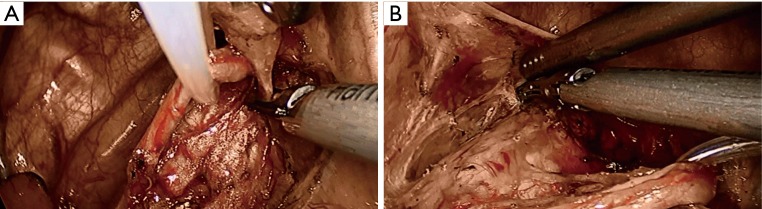
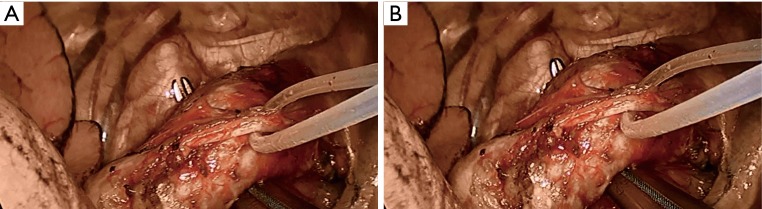
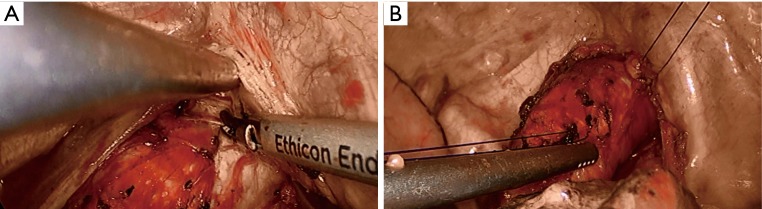
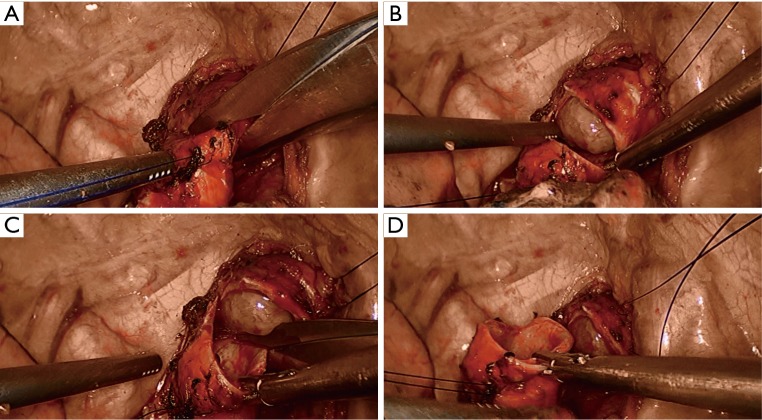
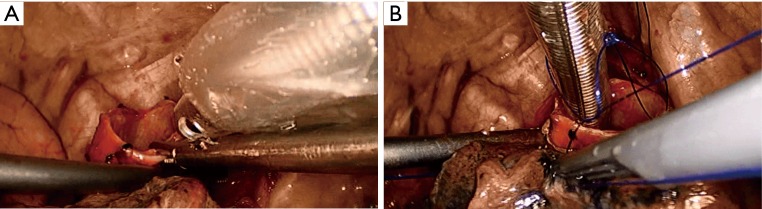
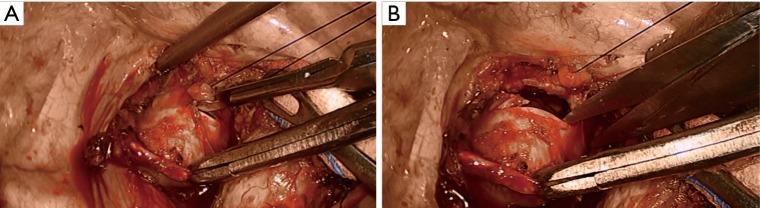
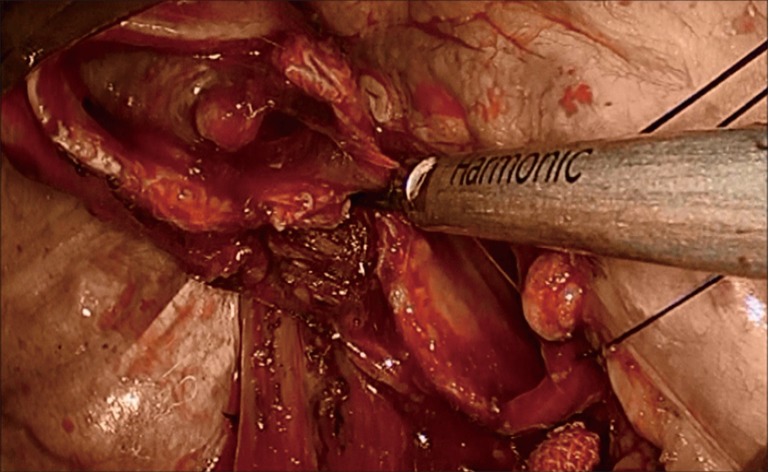
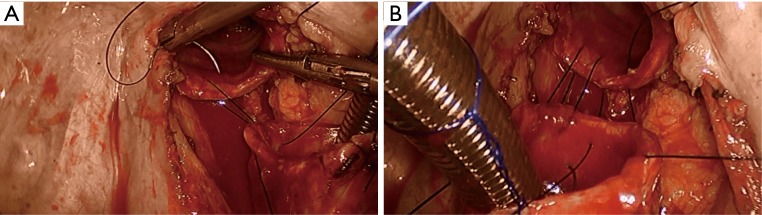
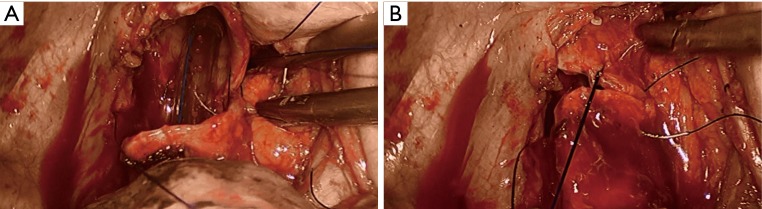
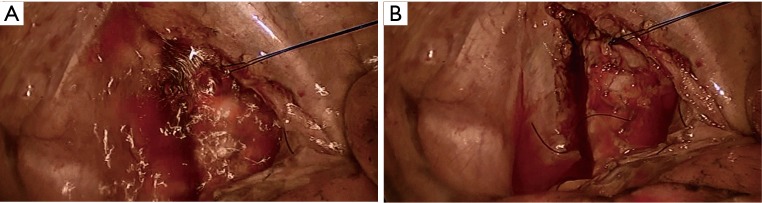
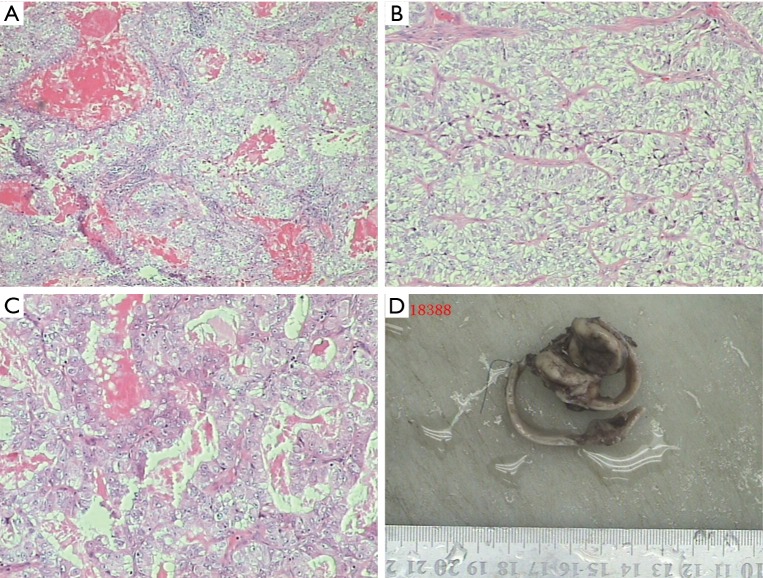
Intratracheal tumor is a rare tumor, accounting for only 2% of upper respiratory tract neoplasms. Its symptoms are similar to those of head and neck cancers, including coughing up blood, sore throat, and airway obstruction. The diagnosis of this disease is often based on the findings of fibrobronchoscopy or computed tomography (CT). Surgery remains the treatment of choice for tracheal tumor. In patients with benign neoplasms or if the tumors have limited involvement, fibrobronchoscopic resection of the tumor can be performed. For malignant tumors, however, radical resection is required. In the past, open incision is used during the surgery for tumors located in thoracic trachea. Along with advances in video-assisted thoracoscopic surgery (VATS) minimally invasive techniques and devices, VATS resection and reconstruction of the trachea can achieve the radical resection of the tumor and meanwhile dramatically reduce the injury to the patients. In this article we describe the application of VATS resection and reconstruction of trachea in the management of a tracheal neoplasm.
Keywords: Tracheal tumor; resection; surgery; thoracoscopy; video-assisted; video-assisted thoracoscopic surgery (VATS).
Conflict of interest statement
Figures


Comment in
-
Thoracoscopic tracheal resection and reconstruction: video-assisted thoracoscopic surgery as a "tool" toward minimally invasive surgery.J Thorac Dis. 2017 Sep;9(9):2895-2897. doi: 10.21037/jtd.2017.08.59. J Thorac Dis. 2017. PMID: 29221260 Free PMC article. No abstract available.
-
Confronting the fundamental challenges of airway surgery: a paradigm shift is practically upon us.J Thorac Dis. 2017 Oct;9(10):3670-3671. doi: 10.21037/jtd.2017.09.52. J Thorac Dis. 2017. PMID: 29268371 Free PMC article. No abstract available.
References
-
- Li S, Liu J, He J, et al. Video-assisted thoracoscopic surgery (VATS) resection and reconstruction of thoracic trachea. Asvide 2016;3:157. Available online: http://www.asvide.com/articles/912 - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous