

Revival of impaired lung perfusion after sleeve lobectomy
- PMID: 27076980
- PMCID: PMC4805826
- DOI: 10.21037/jtd.2016.02.17
Revival of impaired lung perfusion after sleeve lobectomy
Abstract
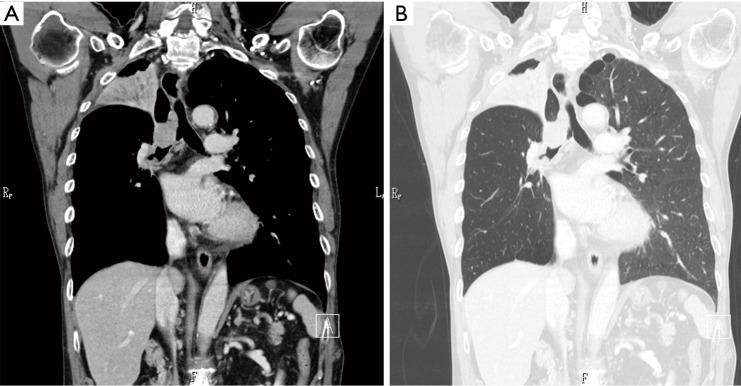
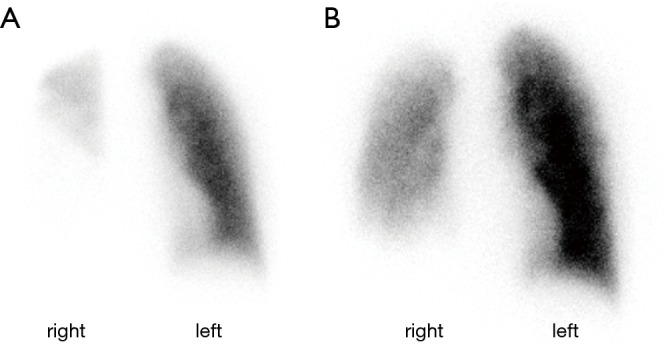
Sleeve resection, a mainstay for centrally-located lung cancer, is a challenging procedure when the preserved lung is impaired. We herein reported a 61-year-old male who underwent right upper sleeve lobectomy for squamous cell carcinoma located at the orifice of the upper bronchus. The tumor invaded the main bronchus. A lung perfusion scan showed severe impairment, while the right middle and lower lobes were well expanded. Not only the spirogram, but also the lung perfusion in the residual lung, had markedly recovered at 2 months after the right upper extended sleeve lobectomy. The patient is currently living his normal daily life. Residual lung perfusion can be revived, even if it is impaired preoperatively.
Keywords: Centrally-located lung cancer; lung perfusion; sleeve resection.
Conflict of interest statement
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources